
Lots of interesting abstracts and cases were submitted for TCTAP 2022. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-167
Percutaneous Transcatheter Closure of Large Spontaneous Ruptured Sinus of Valsalva Aneurysm in a Young Female Patient Using the Amplatzer Duct Occluder
By Krunal Krishnakant Tamakuwala, Abhishek Rajpopat, Vivek Nanda
Presenter
Krunal Krishnakant Tamakuwala
Authors
Krunal Krishnakant Tamakuwala1, Abhishek Rajpopat1, Vivek Nanda1
Affiliation
KD Hospital, India1,
View Study Report
TCTAP C-167
STRUCTURAL HEART DISEASE - Others (Structural Heart Disease)
Percutaneous Transcatheter Closure of Large Spontaneous Ruptured Sinus of Valsalva Aneurysm in a Young Female Patient Using the Amplatzer Duct Occluder
Krunal Krishnakant Tamakuwala1, Abhishek Rajpopat1, Vivek Nanda1
KD Hospital, India1,
Clinical Information
Patient initials or Identifier Number
2021177061
Relevant Clinical History and Physical Exam
A 32‑year‑old female patient, non-diabetic, normotensive with no cardiovascular risk factors presented to the emergency department (ED) of tertiary care hospital with history of complaint of profuse vomiting, chest heaviness, palpitations, perspiration and worsening shortness of breath since yesterday night. On primary survey, on examination, the patient had dyspnea at rest (NYHA class IV) with respiratory rate of 30 per min, room air oxygen saturation of 98%. Echo showed RSOV with 11 mm defect.

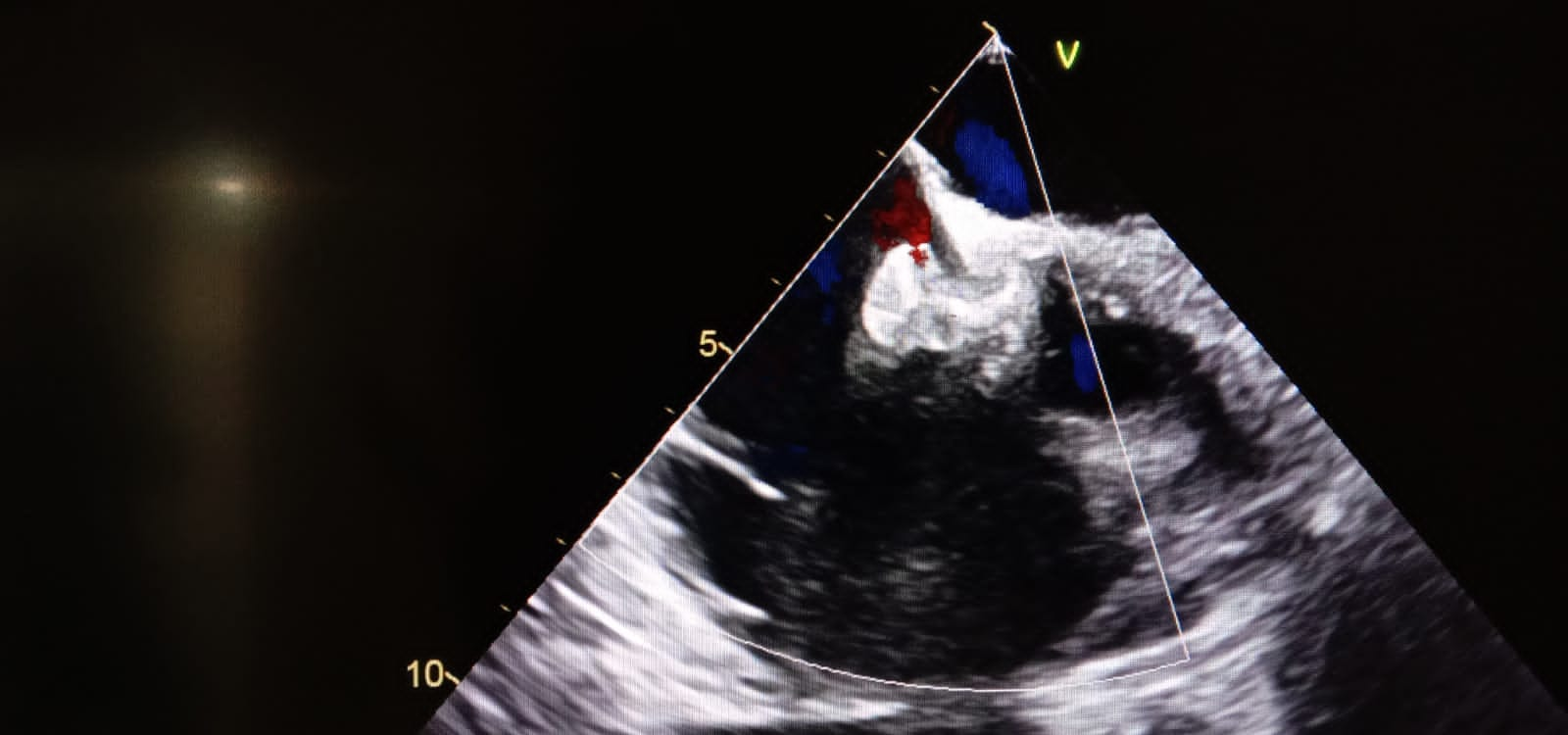
Relevant Test Results Prior to Catheterization
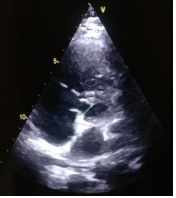
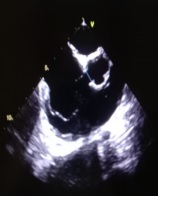
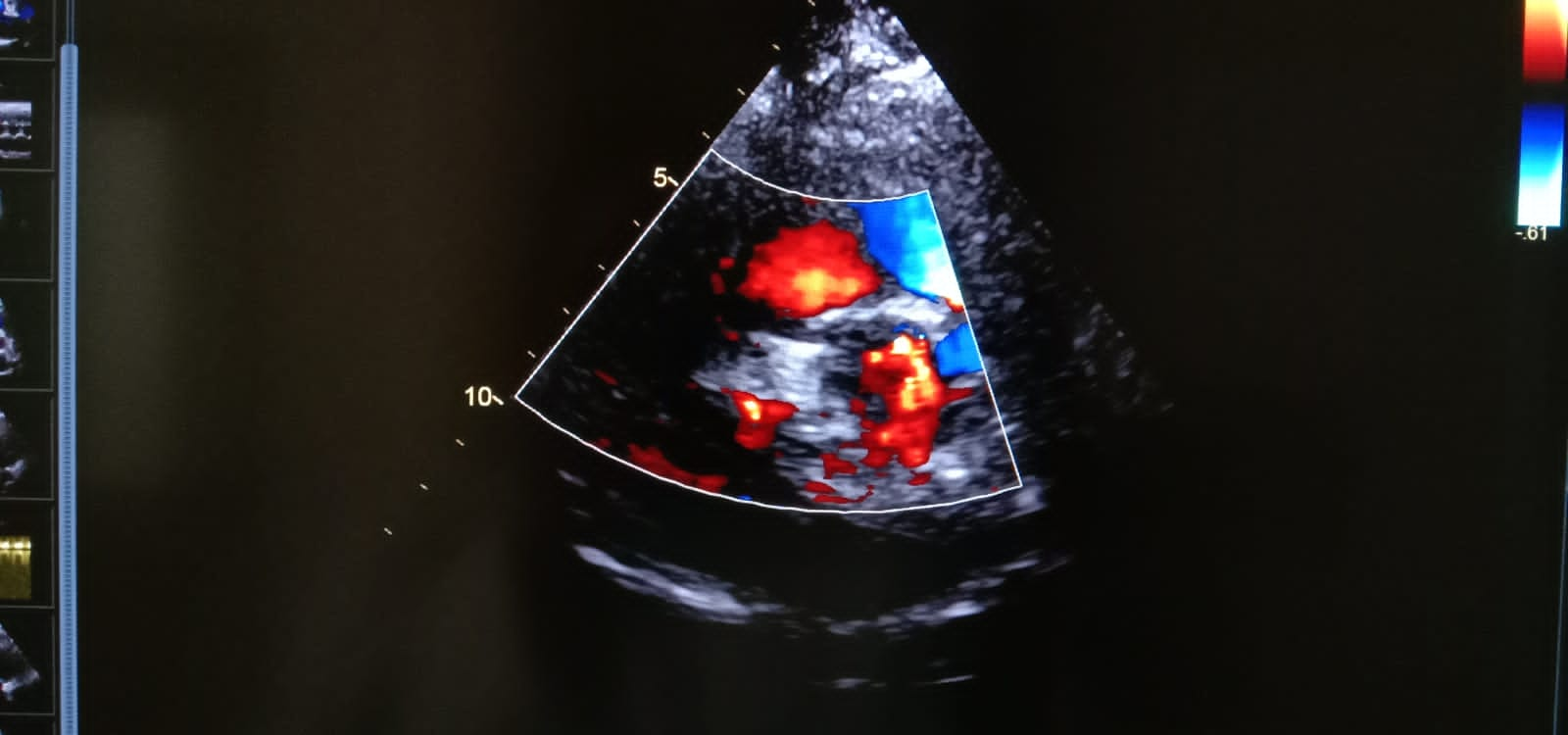
Echo showed RSOV present just above tricuspid valve measuring 10-11 mm. IVC was dilated and non-collapsing. Mild to Moderate TR with Severe PAH, PASP by TR jet is 65 mm hg. No RWMA at rest. Good LV systolic function.
 18c6c3e9-7d6e-499c-9f6c-8c18e987769a.mov
18c6c3e9-7d6e-499c-9f6c-8c18e987769a.mov
52a5da9f-ebbd-43fc-9665-72f57a21a8ed.mov
94e4613b-6e30-4da3-b323-a745c3803539.mov
Relevant Catheterization Findings
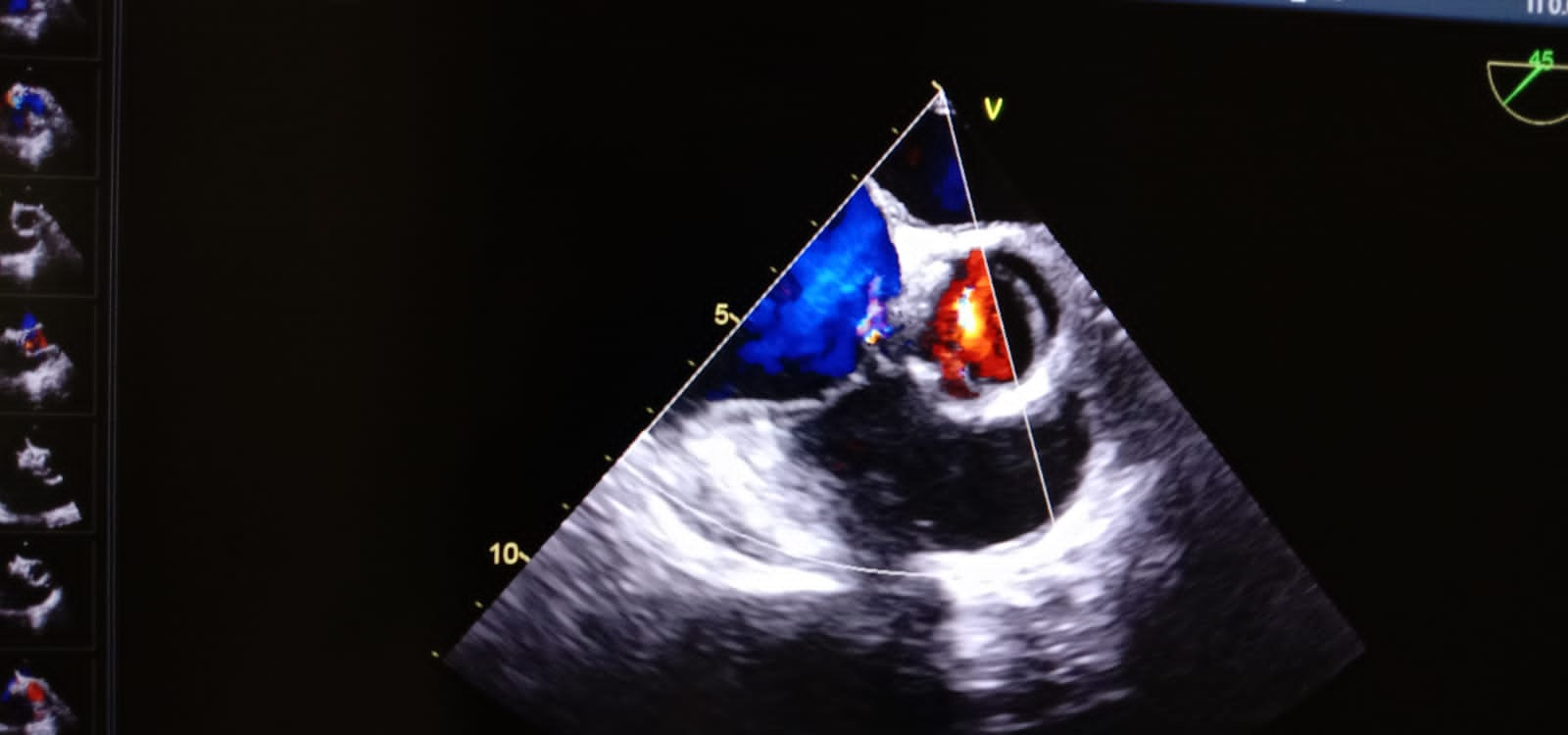
TCC was performed under local anesthesia. Right femoral 5F arterial access and 9F venous access were obtained. Using 5F pigtail catheter through right femoral artery, left ventricular angiogram and aortic root angiogram were performed. A communication between non-coronary sinus of Valsalva and right atrium of 11.0 mm. A 16/14 mm Amplatzer PDA occluder was delivered across the defect after confirming its position under fluoroscopy.
Interventional Management
Procedural Step
TCC was performed under local anesthesia. Right femoral 5F arterial access and 9F venous access were obtained. Using 5F pigtail catheter through right femoral artery, left ventricular angiogram and aortic root angiogram were performed. A communication between non-coronary sinus of Valsalva and right atrium of 11.0 mm. The defect was crossed from right femoral artery using 5F Multipurpose right coronary catheter and angled hydrophilic guidewire (Terumo co-operation, Tokyo, Japan). Initial wire was replaced with exchange length 0.035 in. × 260 cm Teflon guidewire. Exchange length guidewire was manipulated into superior vena cava and snared using Goose Neck snare. Exchange length wire was exteriorized through right femoral vein forming an arterio-venous loop. Over the loop from right femoral vein, 9F Amplatzer TorqVue 45' Delivery system (Amplatzer Duct Occluder, Abbott, USA) was placed across RSOV defect. A 16/14 mm Amplatzer PDA occluder (Amplatzer Duct Occluder, Abbott, USA) was delivered across the defect after confirming its position under fluoroscopy. The entire procedure was done under guidance of TEE. Post procedure, TEE revealed a minimal residual flow across the device. No paravalvular leak.
00bfab9c-8626-4f96-97c7-23bda59867c8.mov
a57ce9e1-8c8b-47e6-b443-299ed7c37c7d.mov
b8991880-aa13-4623-b250-91030613fae9.mov
f9e9dd1a-54e8-4f4c-9c19-eca54b555d8a.mov
Case Summary
RSOV aneurysm is a rare cardiac deformity that carries a severe prognosis. Transthoracic echocardiogram is sufficient to accurately diagnose this condition.
TCC of RSOVA is safe, effective and can be performed for bigger defect (> 11 mm) using Amplatzer PDA occluder. PDA device Occluder is an economical modality of treatment with good short-term and intermediate outcomes. In carefully selected patients this provides an attractive alternative to surgical closure, thereby avoiding the inherent morbidity of sternotomy and cardiopulmonary bypass.
TCC of RSOVA is safe, effective and can be performed for bigger defect (> 11 mm) using Amplatzer PDA occluder. PDA device Occluder is an economical modality of treatment with good short-term and intermediate outcomes. In carefully selected patients this provides an attractive alternative to surgical closure, thereby avoiding the inherent morbidity of sternotomy and cardiopulmonary bypass.