
Lots of interesting abstracts and cases were submitted for TCTAP 2022. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-071
Crush Stenting at Nodular Calcified Left Main Bifurcation Lesion
By Achmad Fauzi Yahya, Sanggam Sinambela
Presenter
Sanggam Sinambela
Authors
Achmad Fauzi Yahya1, Sanggam Sinambela1
Affiliation
Dr. Hasan Sadikin Central General Hospital, Indonesia1,
View Study Report
TCTAP C-071
CORONARY - Complex and Higher Risk Procedures for Indicated Patients (CHIP)
Crush Stenting at Nodular Calcified Left Main Bifurcation Lesion
Achmad Fauzi Yahya1, Sanggam Sinambela1
Dr. Hasan Sadikin Central General Hospital, Indonesia1,
Clinical Information
Patient initials or Identifier Number
Mr. S
Relevant Clinical History and Physical Exam
A 67-year-old male presented with Stable Angina Pectoris Canadian Cardiovascular Society class II. Five months prior to admission, he had Primary Percutaneous Coronary Intervention (PCI) with Plain Old Ballloon Angioplasty (POBA) at calcified LAD due to ST segment elevation myocardial infarction (STEMI) extensive anterior wall in another hospital. His coronary risk factor was smoker. Physical examination showed unremarkable results.
Relevant Test Results Prior to Catheterization
His laboratory results were within normal limits. The baseline ECG was sinus rhythm with old anterior myocardial infarction. Echocardiogram showed LVEF 37% with akinetic of mid-apicoanterior, anteroseptal, inferoseptal, and inferior; hypokinetic of all basal segments, basal-mid anterolateral, inferolateral. Nuclear Perfusion Scan showed inducible ischemia at basal-anterior, parts of basal-anterolateral, basal-mid.
Relevant Catheterization Findings
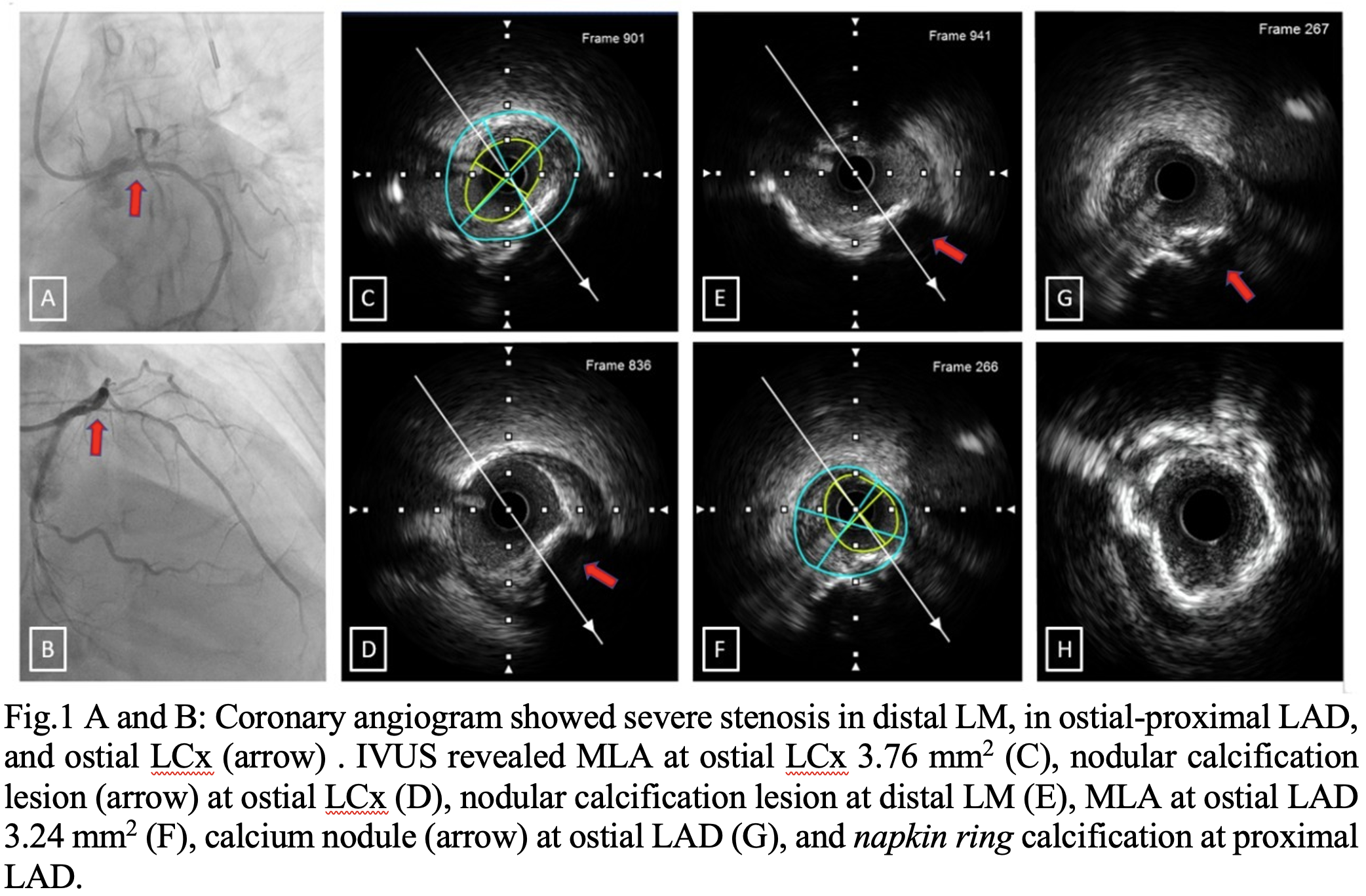
Angiogram (Figure 1) revealed moderate stenosis and severe calcification at distal LM (Medina 1,1,1); severe stenosis and severe calcification at ostial-proximal LAD, critical stenosis at proximal LAD; moderate stenosis with severe calcification at ostial LCx; diffuse stenosis and severe calcification at ostial to distal RCA, with severe stenosis at proximal RCA. We decided to perform PCI to LM bifurcation lesion.
 Video 1 LCX-IVUS-Pre-stenting.mov
Video 1 LCX-IVUS-Pre-stenting.mov
Video 2 LAD-IVUS-pre-stenting.mov
Interventional Management
Procedural Step
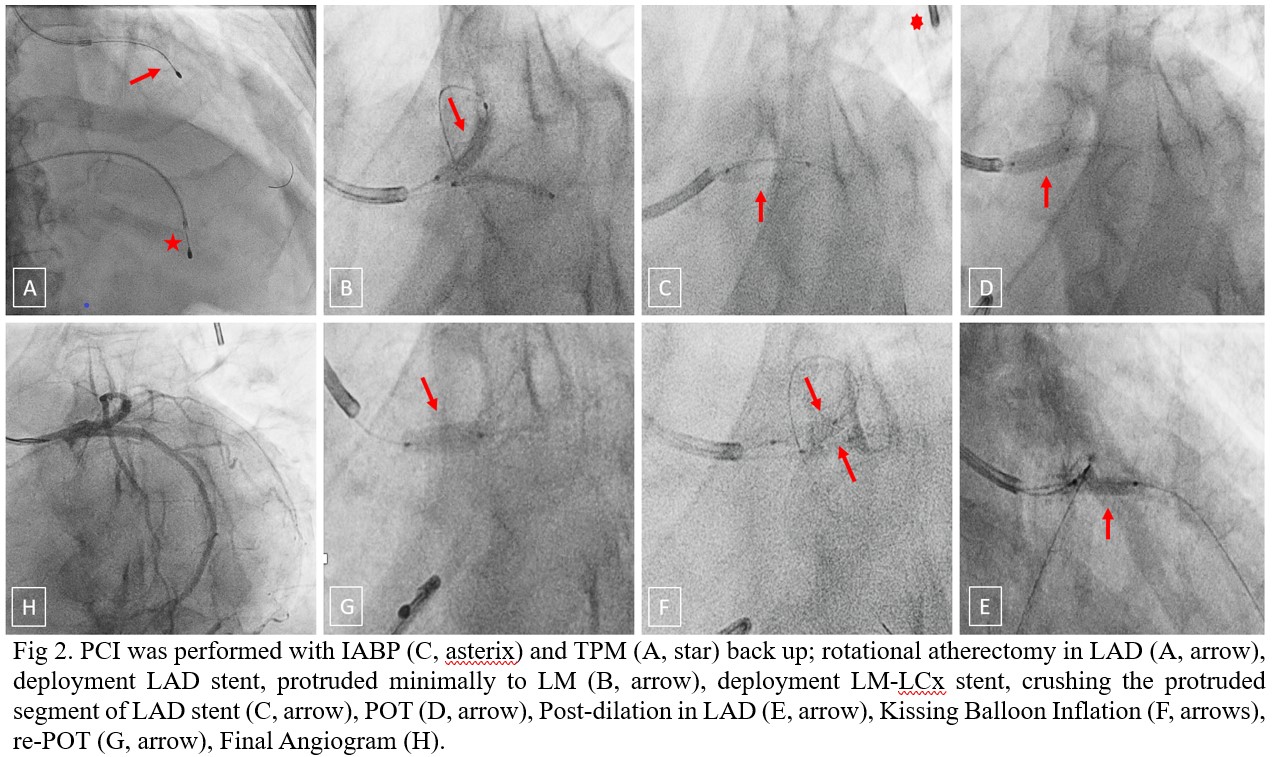
Procedure was backed up with IABP and TPM. A 7 Fr GC 3.5 was inserted via Left Distal Transradial access, followed by wiring to LAD and LCx. IVUS (Boston Scientific, USA) was performed to both LCx-LM (Video 1) and LAD-LM (Video 2) which revealed nodular calcification at ostial-proximal LCx, calcified nodule at ostial LAD, napkin ring at proximal LAD, and nodular calcification at distal LM (Fig 1). Rotational Atherectomy (RA) was performed at LAD using Rotalink Plus burr 1.75 mm (Boston Scientific, USA) at speed 170k rpm, afterward using Cutting Balloon (CB) Wolverine 2.5/10 mm (Boston Scientific, USA) at LAD and LCx. IVUS post-RA and CB (Video 3) showed multiple cracks. We decided to perform crush stenting. Stent Xience Prime 2.75/28 mm (Abbott Vascular, USA) deployed at LAD (protruded minimally to LM), and then stent Xience Prime 3.5/18 mm deployed at LM-LCx, crushing the protruded LAD stent (Fig 2), followed by POT with Simpass NC balloon 4.5/15 mm (Simeks Medical, Turkey) at 18 atm. Post-dilation at LAD with NC Balloon Raiden 2.75/15 mm (Kaneka Medical, Japan), followed by kissing balloon inflation (KBI) with NC balloon Raiden 3.5/10 mm at LM-LCx and NC balloon Raiden 2.75/15 mm at LM-LAD, and then re-POT. Final angiogram showed TIMI 3 flow. Final IVUS in LM-LCx (Video 4) showed well-expanded and well-apposed stent, MSA 10 mm2 at proximal LCx, and MSA 14.6 mm2 at LM. After 3 months of follow-up, the angiogram revealed stent patent in situ at LM-LCx and LAD.
Video 3 LAD-post-RA-Cutting-balloon.mov
Video 4 LM-LCx-Final-IVUS-Evaluation.mov
Case Summary
Left Main bifurcation lesions pose challenging situation to perform PCI, let alone when the lesion is severely calcified, particularly nodular calcified lesion. Intravascular imaging-guided lesion preparation remains the cornerstone for good results of stent expansion and apposition for such case. Two-stent technique, including crush stenting, could be considered as the treatment strategy.