
Lots of interesting abstracts and cases were submitted for TCTAP 2022. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-099
Incidental Complication After Successful Revascularization of Chronic Total Occlusion
By Yen-Ting Lu, Tsung-Yu Ko
Presenter
Yen-Ting Lu
Authors
Yen-Ting Lu1, Tsung-Yu Ko2
Affiliation
Taipei City Hospital Renai Branch, Taiwan1, National Taiwan University Hospital, Taiwan2,
View Study Report
TCTAP C-099
CORONARY - Complications
Incidental Complication After Successful Revascularization of Chronic Total Occlusion
Yen-Ting Lu1, Tsung-Yu Ko2
Taipei City Hospital Renai Branch, Taiwan1, National Taiwan University Hospital, Taiwan2,
Clinical Information
Patient initials or Identifier Number
6833822
Relevant Clinical History and Physical Exam
A 55-year-old man had history of diabetes mellitus and hypertriglyceridemia for one year and was followed up at local medical department. He suffered from exertional chest tightness & dyspnea when he was climbing stairs of five stories since 05/2020. These discomforts gradually worsened in recent one year. The myocardial perfusion imaging showed reversible perfusion defects at anterior territory. No specific physical abnormality was found. He was referred for coronary angiography.
Relevant Test Results Prior to Catheterization
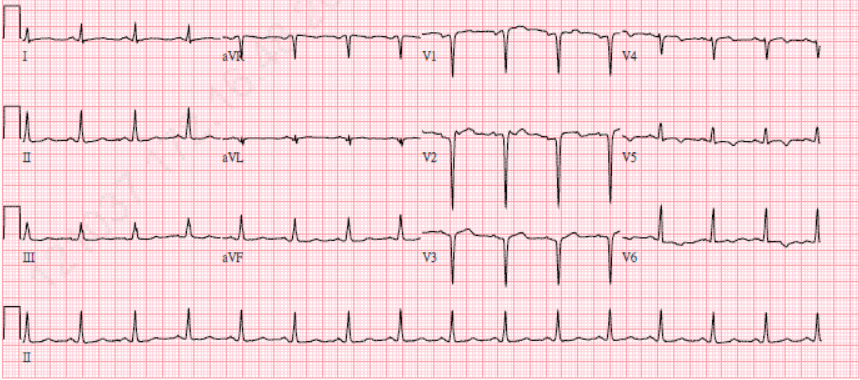
The myocardial perfusion imaging at local medical department showed reversible perfusion defects at anterior territory. The 12-lead electrocardiogram showed normal sinus rhythm with QS pattern at precordial V1-V3 lead, suspected old anteroseptal infarction. Chest x-ray showed normal heart size, atherosclerosis of aorta with calcification without no definite active lung lesions.

Relevant Catheterization Findings
Coronary angiography was performed from left radial arterial access. Patent left main & left circumflex artery. Left anterior descending artery (LAD) had 80% stenosis at proximal part, and chronic total occlusion since middle part with bridging & septal collateral channel to distal part of LAD. Right coronary artery (RCA) had 70% stenosis at proximal part, 50% stenosis at middle part, 70% stenosis at distal part, 90% stenosis at PLA. RCA had epicardial & septalcollateral channel to LAD.
 2022 TCTAP Case - CAG part.mp4
2022 TCTAP Case - CAG part.mp4
Interventional Management
Procedural Step
Step 1: We used Asahi Sion Blue with microcatheter Finecross but failed to cross mLAD CTO proximal cap.Step 2: Keep antegrade wire escalation (AWE) strategy by Asahi Filter XT-A but all failed to cross proximal cap.Step 3: Keep antegrade wire escalation (AWE) strategy by Asahi GAIA second with success to cross distal cap and reach the distal true lumen.Step 4: Used IVUS to confirm luminal diameter & stenosis severity.Step 5: Sequential balloon angioplasty to mLAD CTO by 1.5*15 mm, 2.0*1.5 mm, and by cutting balloon as Scoreflex 2.5*10 mm .Step 6: We deployed "Terumo Ultimaster 2.5*38 mm" to mLAD, and deployed "Terumo stent Ultimaster 3.0*28 mm" to pLAD.Step 7: Hypotension with subintimal dissection over LM-LCX was confirmed by angiography. Deployed DES3 "Terumo stent Ultimaster 3.5*15 mm" to LM-LAD.Step 8. Used thrombosuction "Terumo ELIMINATE Aspiration catheter 7FR" to LM-LCX, with several white thrombus.Step 9: Implanted IABP via LFA due to unstable hemodynamics.Step 10: We deployed "Terumo Ultimaster 3.5*24 mm" to LM-LCX, and IC tirofiban administration .Step 11: Kissing balloon for LM bifurcation lesion. Step 12: Final angiogram showed improved blood flow without residual thrombus (TIMI 3 flow), so we closed the examination and transferred the patient to CCU for further treatment.
TCTAP PCI-1 high.mp4
TCTAP PCI-2 high.mp4
Case Summary
The intimal dissection and acute thrombus formation may be seen during percutaneous coronary intervention. The coronary intima may be injured by balloon angioplasty and stent deployment, which was very common intervention in this era. We share this special case as combined intravascular imaging usage with dedicate problem-solving strategy, which can help us to differential the no-reflow phenomenon between dissection or thrombosis, even the clinical condition is life-threatening.