
Lots of interesting abstracts and cases were submitted for TCTAP 2022. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-047
Rota Ablation in Heavily Calcified LM Bifurcation Lesion
By Raghav Sharma, Karan Dang, Dr Asees Paul Singh, Sudhir Mor
Presenter
Raghav Sharma
Authors
Raghav Sharma1, Karan Dang2, Dr Asees Paul Singh3, Sudhir Mor4
Affiliation
RKM Hospital, India1, Artemis Ascoms, India2, Fortis Hospital Mohali, India3, Ravindra Hospital, India4,
View Study Report
TCTAP C-047
CORONARY - Bifurcation/Left Main Diseases and Intervention
Rota Ablation in Heavily Calcified LM Bifurcation Lesion
Raghav Sharma1, Karan Dang2, Dr Asees Paul Singh3, Sudhir Mor4
RKM Hospital, India1, Artemis Ascoms, India2, Fortis Hospital Mohali, India3, Ravindra Hospital, India4,
Clinical Information
Patient initials or Identifier Number
MRS R
Relevant Clinical History and Physical Exam
55-year-old female, known case of Hypertension presented with history of DOE NYHA functional class II increased on exertionpast H/o : k/c/o DM for 10 years, no H/O CAD, k/c/o HTN X 12 YEARS personal H/O : Non-smoker , Non-alcoholicphysical examination : vitals stable, JVP not elevated CV: S1S2 +, no murmur RS: NVBS+Other systems were normal
Relevant Test Results Prior to Catheterization
All labs were remarkable.EKG: NSR changes consistent with old AWMI.ECHO: APICAL SEPTUM, MID SEPTUM AND APICO LATERAL WALL SEVERELY HYPOKINETIC WITH MOD LV DYSFUNCTION WITH LVEF OF 40%
Relevant Catheterization Findings
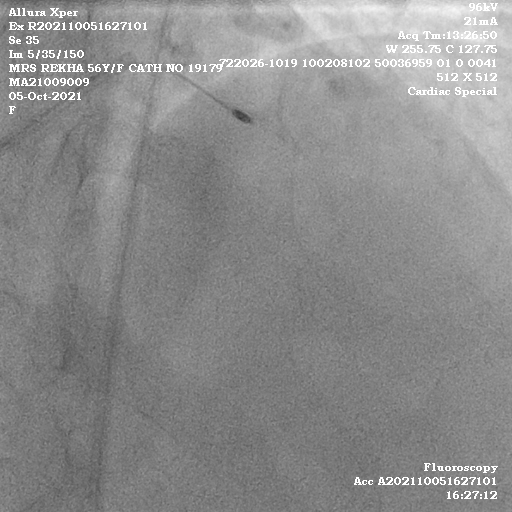
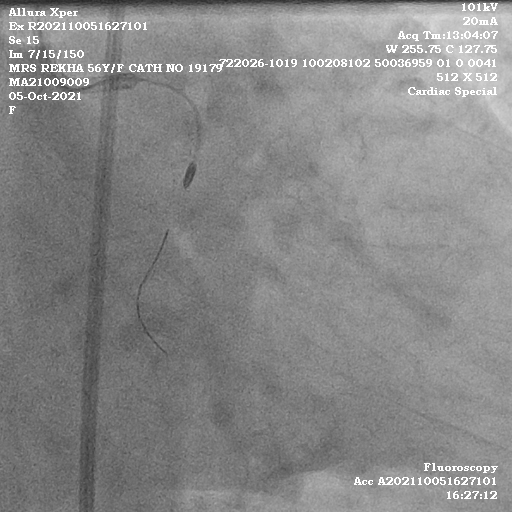
CAG: Left Main calcified Distal LMCA 70-80% Stenosis.LAD Type C vessel. Ostio proximal tubular disease upto 99% with heavy calcification, Mid Distal LAD 70-80% tubular disease.LCX Dominant vessel Ostioproximal 70-80% Tubular disease with calcification, Distal LCX 70% Discrete stenosis.Obtuse Marginal 1 Ostioproximal tubular 80-90% disease.RCA Non Dominant vessel proximal to distal diffuse disease up to 80-90%.Calcific Distal Left Main TVD with Medina 1,1,1.



Interventional Management
Procedural Step
Right femoral access was taken. EBU 7 Fr guide was engaged in LM. Fielder FC 0.014 wire was parked in distal LCX. Wire could not be parked in LAD as LM was diseased and calcified. OTW Finecross Microcatheter was parked in distal LCX. Fielder FC wire was exchanged with 0.009 ROTA exchange length wire and parked in distal LCX. Finecross was removed. OTW 1.5 ROTA burr was taken and rotablation was done at 1,80000 RPM from LM to Mid LCX. After 2-3 runs, burr crossed the lesion. Then wire and burr were removed. Then Fielder FC was parked in distal LAD and using Finecross ROTA wire was exchanged. Same 1.5 burr was taken and 2-3 runs were done in LM-LAD. ROTA wire was exchanged with Fielder FC and 2nd Fielder FC was parked in Distal LCX. Both vessels were dilated with 2.5 mm Semi-compliant balloons up to 15 atm. 4x40 mm DES was deployed in LM-LCX at 14 atm with wire jailed in LAD. Subsequently wire was removed from LAD and repositioned across the struts and parked in distal LAD. LCX was dilated with 4x12 mm NC @15 atm and LM WITH 4.5X12 mm @15 atm. Now over LAD wire 1.5 NC and subsequently 2.5 NC were taken and struts were dilated. 2nd DES 3X40 mm was deployed across the struts of LM-LCX stent with 1 mm struts protruding in LM-LCX stent. Now with 2 balloons 4x12 mm NC and 3x12 NC were taken and FKB was done. LAD was dilated with 3x12 mm throughout its length. A good TIMI III flow was noted with no complications. Patient was discharged after 2 days.

 36 sec.avi
36 sec.avi
Case Summary
PTCA in a densely calcified Left main triple vessel disease is always a challenge, especially when diffuse disease where putting graft is not possible due to poor targets. A thorough understanding of anatomy is essential as calcified arteries always are fragile and need careful handling use of technology. Especially rotablation is a good tool but conceptual understanding is a must. From our case points which are clear are:1) quick decision making and clear anticipation of complication and their management is a must to attempt this case.2) technically sound mind and hand are required specially knowing concepts about rota is a must.