
Lots of interesting abstracts and cases were submitted for TCTAP 2022. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-044
Percutaneous Coronary Intervention in a Complex Left Main Trifurcation Lesion Using Two Guide Catheters
By Harinder K. Bali, Amreen Dhindsa
Presenter
Harinder K. Bali
Authors
Harinder K. Bali1, Amreen Dhindsa2
Affiliation
Paras Hospitals, India1, Fortis Hospital, India2,
View Study Report
TCTAP C-044
CORONARY - Bifurcation/Left Main Diseases and Intervention
Percutaneous Coronary Intervention in a Complex Left Main Trifurcation Lesion Using Two Guide Catheters
Harinder K. Bali1, Amreen Dhindsa2
Paras Hospitals, India1, Fortis Hospital, India2,
Clinical Information
Patient initials or Identifier Number
RR
Relevant Clinical History and Physical Exam
76-year-old female presented with angina and dyspnea on exertion since the past 1 month, progressing to NYHA class 3 since past 2 days.Past history was significant for diabetes mellitus.Physical examination revealed normal first and second heart sound with no added sounds and murmurs.
Relevant Test Results Prior to Catheterization
ECG: T wave inversions from V1-V6Echocardiography: regional wall motion abnormality present in anterior wall, with moderate mitral regurgitation and a left ventricular ejection fraction of 50%.
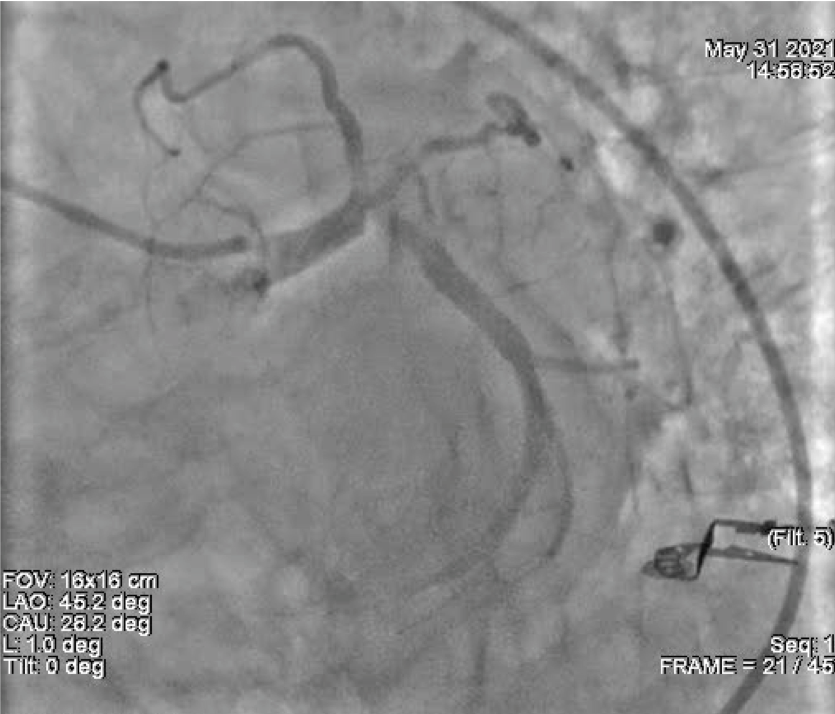
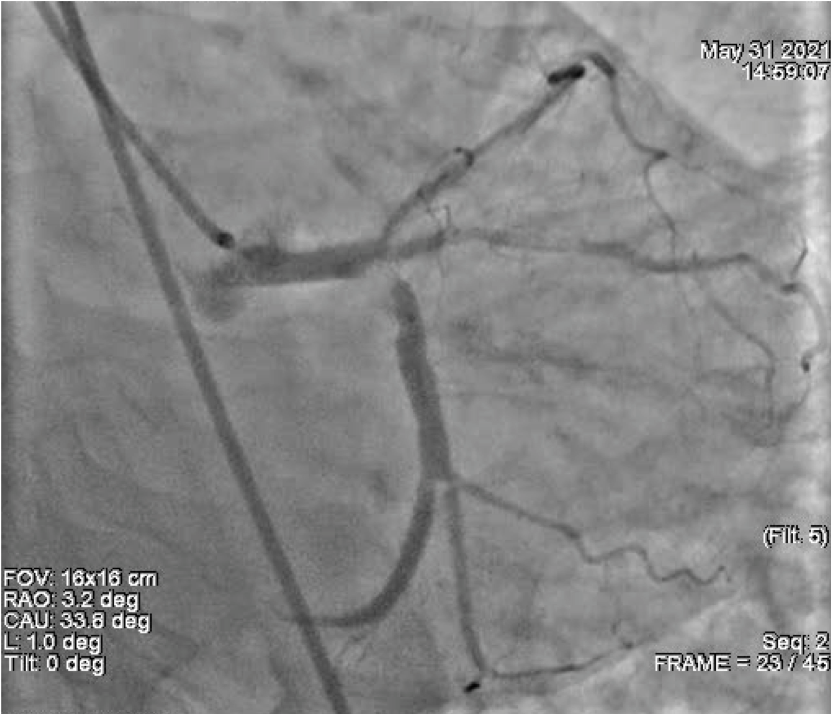
Relevant Catheterization Findings
Route: Right Femoral Anesthesia: Xylocaine Hardware:6F JR 3.5, 6F JL 4.0 Contrast: Ornnipaque CORONARY PROFILE LM: Distal segment calcification noted involving ostium of LCx LAD:Type III vessel. ostial 70-80% stenosis, mid and distal segment are normal. Diagonal: NormalRamus: Normal LCx: Dominant, ostial calcific lesion with 99% stenosis. OM: Normal RCA: Non Dominant, Normal PDA: Normal PLV: Normal
Interventional Management
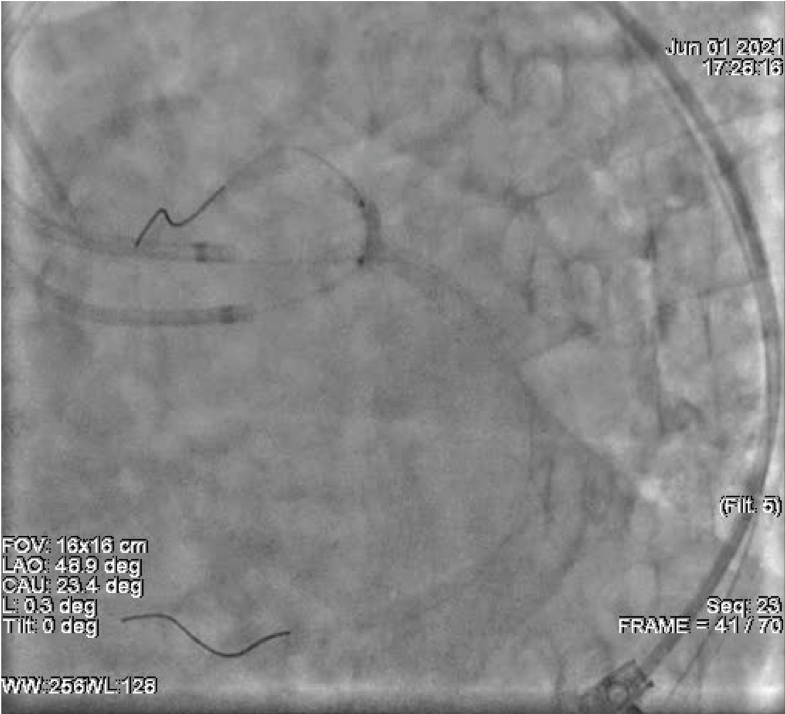
Procedural Step
PCI of left main trifurcation done using TAP technique, 2 guide catheters used.


Route: Right/Left Femoral Artery
Contrast: Omnipaque
Anesthesia: 2% Xylocaine (Local Anesthesia)
Guiding Catheter: 7F EBU 3.5, 6F EBU 3.5 Guiding Wire: Fielder XT,BMW (3)
Balloon: Pre stent dilatation done with 2.0x15 mm, 2.5x15 mm, 3.0x15 mm balloons
Stent: RESOLUTE ONYX stent 4.0x30 mm deployed in LM to LCx; XIENCE XPEDITION stent 2.75x23 mm deployed in proximal LAD
Balloon: Post stent dilatation done with 2.5x12 mm, 2.75x15 mm, 3.0x12 mm, 4.0x15 mm, 5.0x8 mm NC balloons, Kissing Balloon dilation of trifurcation done with 2.75x15 mm (LAD) ,2.5x12 mm (Ramus), 3.0x12 mm (LCx) ,POT done with 5.0x8 mm (LM)
Additional Drug: Heparin 7500 units
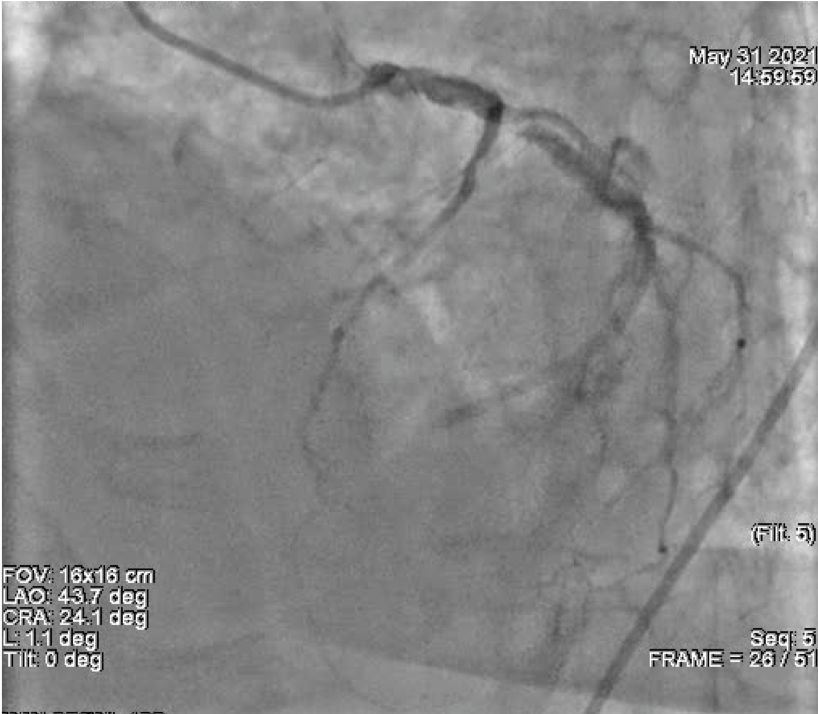
Case Summary
Successful PTCA and stenting of LM-->LCx, LAD and POBA to ramus intermedius done.Left main trifurcation lesions are complex lesions requiring expertise in intervention, and good results can be achieved by applying rules of bifurcation stenting to trifurcation lesions.