
Lots of interesting abstracts and cases were submitted for TCTAP 2022. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-113
The Stubborn LAD
By Nanda Iryuza, Arwin Saleh Mangkuanom
Presenter
Nanda Iryuza
Authors
Nanda Iryuza1, Arwin Saleh Mangkuanom1
Affiliation
National Cardiovascular Center Harapan Kita, Indonesia1,
View Study Report
TCTAP C-113
CORONARY - Complications
The Stubborn LAD
Nanda Iryuza1, Arwin Saleh Mangkuanom1
National Cardiovascular Center Harapan Kita, Indonesia1,
Clinical Information
Patient initials or Identifier Number
2021494059
Relevant Clinical History and Physical Exam
A 59-year-old female with chief complain of angina on exertion since 2 years before admission. Breathlessness and orthopnea were denied. Patient was hypertensive with routine once daily anti-hypertensive drugs consumption of 16 mg candesartan. Physical examination was unremarkable, except for elevated blood pressure to 157/91 mmHg.
Relevant Test Results Prior to Catheterization
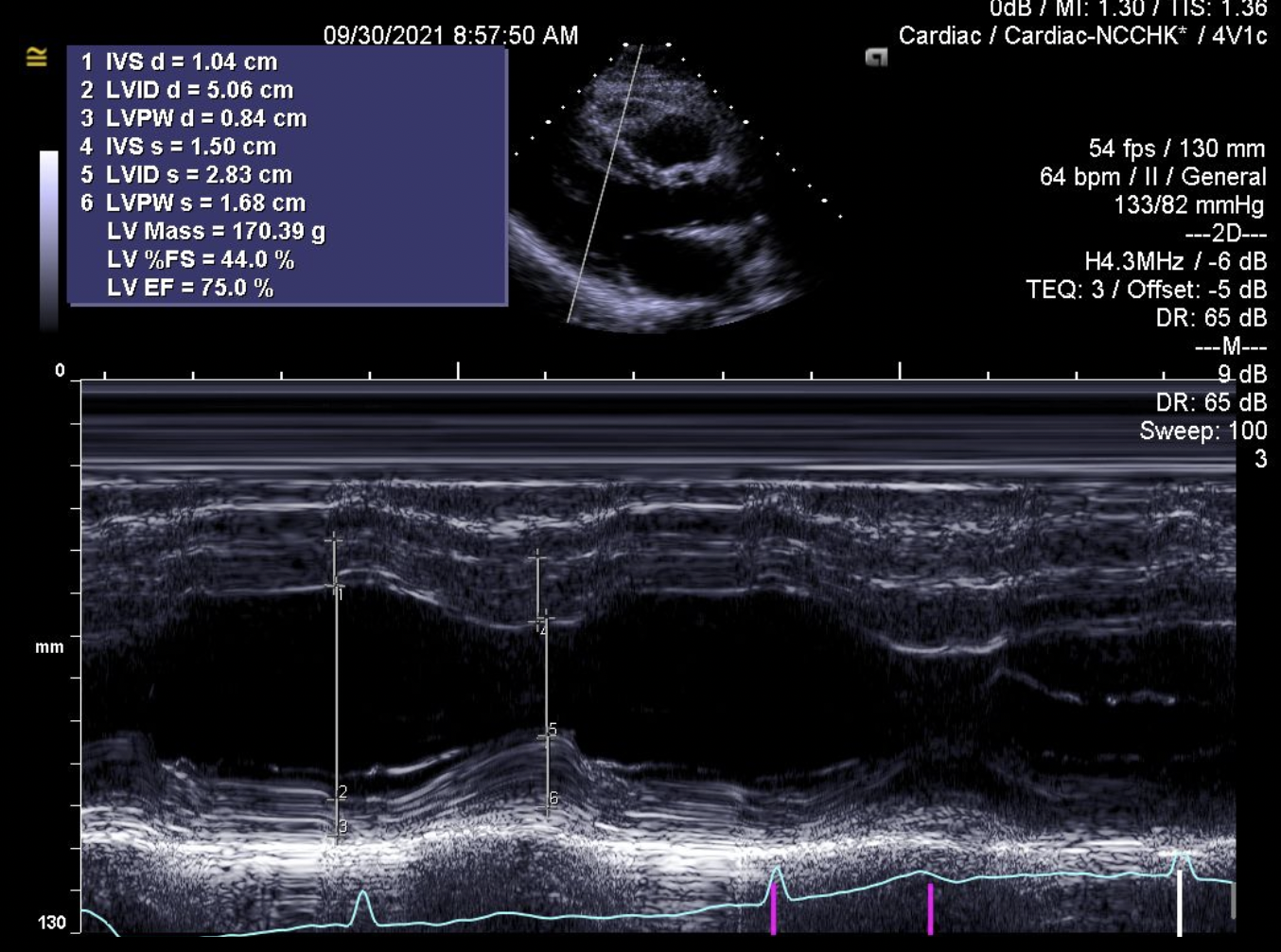
High level of LDL was reported from laboratory result. Resting ECG revealed normal sinus rhythm with left ventricular hypertrophy and no ST segment nor T wave changes. Echocardiography shown normal ejection fraction of 62% and no valvular abnormalities. Additionally, positive ischemic result was reported from the exercise stress test.
 echo plax.mov
echo plax.mov
Relevant Catheterization Findings
Left coronary angiography revealed normal left main vessel, chronic total occlusion at the proximal LAD, and normal LCx. In addition, right coronary angiography shown moderate stenosis at the mid part, and distal part of LAD was collateralized by RCA. Calculated SYNTAX score 1 was 20.5, and calculated JCTO score was 1.
CTO LAD dual injection.mov
dissect caudal edit.mov
dissect spider.mov
Interventional Management
Procedural Step
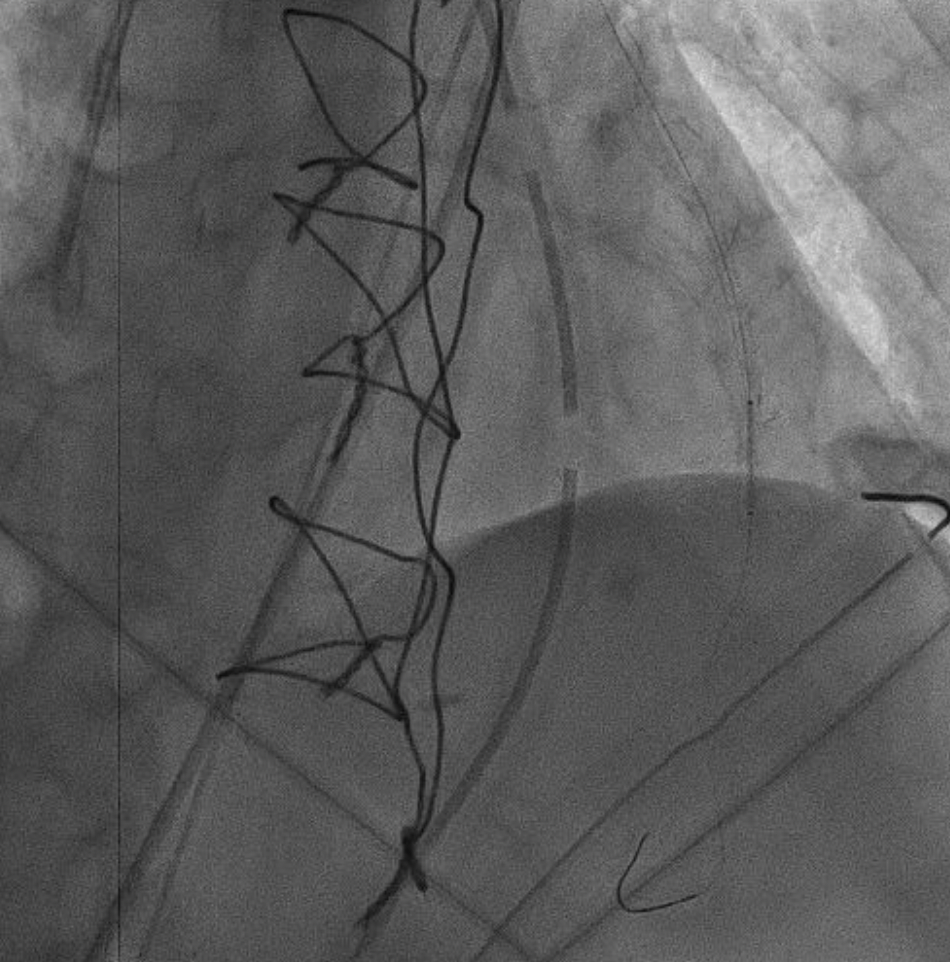
Patient was reported suffering from cardiac arrest 1 day after CABG surgery. ECG showed recurrent ventricular tachycardia and was stabilized by 200 J unsynchronized defibrillation. Echocardiography shown decreased ejection fraction to 31% with new regional wall motion abnormality and reduction of stroke volume and cardiac output. IABP insertion was performed before the patient was sent back to catheterization lab. Angiography was performed and shown occluded LIMA to LAD graft with TIMI 0 flow. Using 6F IMA guide catheter, Sion Blue wire could not cross the lesion. Wire was escalated to Fielder XTA and successfully crossed the lesion. Sion Blue wire was advanced from LIMA to distal LAD and Fielder XTA was pulled out. Lesion was pre-dilated with Maverick 2.0/15 mm balloon up to 10 atm along the LIMA graft. However, the flow was not restored after several pre-dilatation. Thrombus aspiration was done using Eliminate catheter, and LIMA to LAD flow restored after the aspiration. Then, DES Promus Premier 2.5/38 mm was deployed at the anastomosis of LIMA and LAD up to 14 atm. Post-stent deployment angiography revealed non-flow limiting dissection and Ellis type III perforation at the stent implantation site. Therefore, Bentley Be-Graft stent graft 2/5/12 mm was deployed up to 12 atm at the perforation site. Final angiography showe sealed perforation, no thrombus, and mild non-flow limiting dissection at the mid LIMA graft.
occluded LIMA-LAD.mov
perforation.mov
sealed perforation.mov
Case Summary
In conclusion, unsuccessful CTO PCI procedure may result in several complications such as coronary dissection and perforation. The bail out strategy might range from postponing the PCI procedure to CABG surgery. Although internal mammary artery is the best vessel for bypassing the LAD, graft failure can be presented in some cases. PCI procedure attempt to the bypass graft vessels may result in a number of complications especially SVG PCI. Therefore, PCI to SVG might be the last option after PCI to native vessels and LIMA. In this case, LIMA to LAD perforation might be happened due to stent implantation pressing the anastomosis site, and was successfully sealed with the stent graft.