
Lots of interesting abstracts and cases were submitted for TCTAP 2022. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-132
Incidentally Detected Overlooked Coarctation of Aorta During Cerebral Angiography
By Yusuf Ziya Sener, Ahmet Hakan ATEŞ, Mehmet Levent Sahiner, Ergün Baris Kaya, Enver Atalar, Tevfik Karagöz, Kudret Aytemir
Presenter
Yusuf Ziya Sener
Authors
Yusuf Ziya Sener1, Ahmet Hakan ATEŞ2, Mehmet Levent Sahiner2, Ergün Baris Kaya2, Enver Atalar2, Tevfik Karagöz2, Kudret Aytemir2
Affiliation
Beypazarı State Hospital, Turkey1, Hacettepe University Faculty of Medicine, Turkey2,
View Study Report
TCTAP C-132
ENDOVASCULAR - Aorta Disease and Intervention
Incidentally Detected Overlooked Coarctation of Aorta During Cerebral Angiography
Yusuf Ziya Sener1, Ahmet Hakan ATEŞ2, Mehmet Levent Sahiner2, Ergün Baris Kaya2, Enver Atalar2, Tevfik Karagöz2, Kudret Aytemir2
Beypazarı State Hospital, Turkey1, Hacettepe University Faculty of Medicine, Turkey2,
Clinical Information
Patient initials or Identifier Number
MEU
Relevant Clinical History and Physical Exam
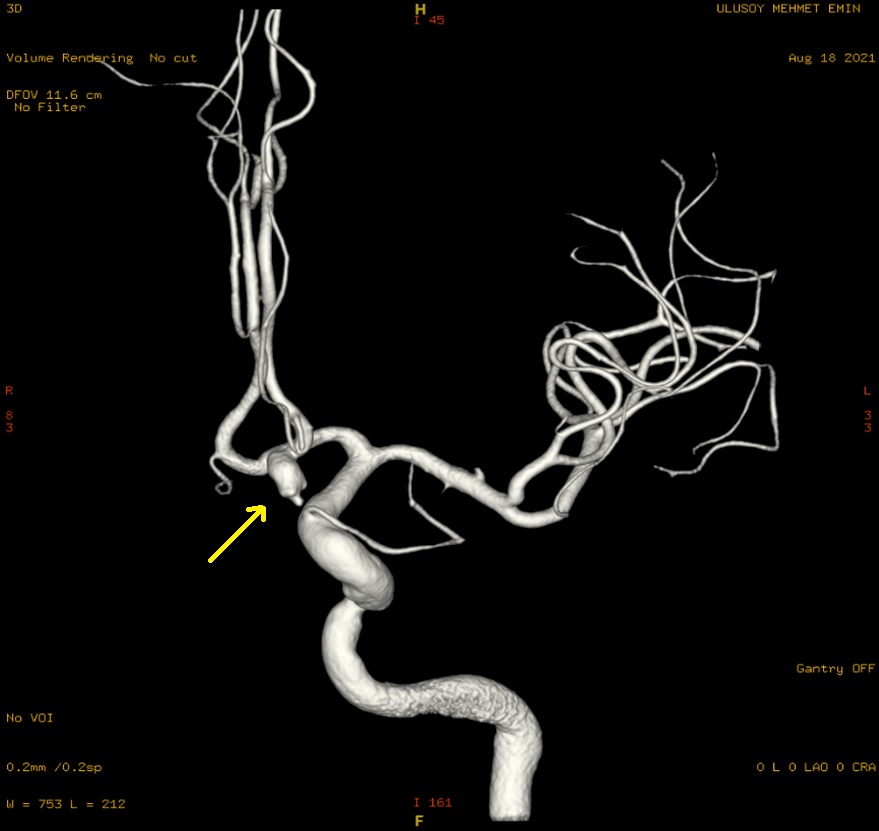
A 57-year-old male with hypertension and coronary artery disease was referred due to incidentally detected coarctation of aorta (CoA). His history revealed that he had undergone CABG 4 years ago due to multi-vessel disorder established by transradial coronary angiography. Peripheral angiography was performed 1 year ago because of bilateral claudication;, however, there was not any significant stenosis in lower extremity arteries. He was admitted with TIA, and brain CT angiography showed ACA aneurysm.
Relevant Test Results Prior to Catheterization
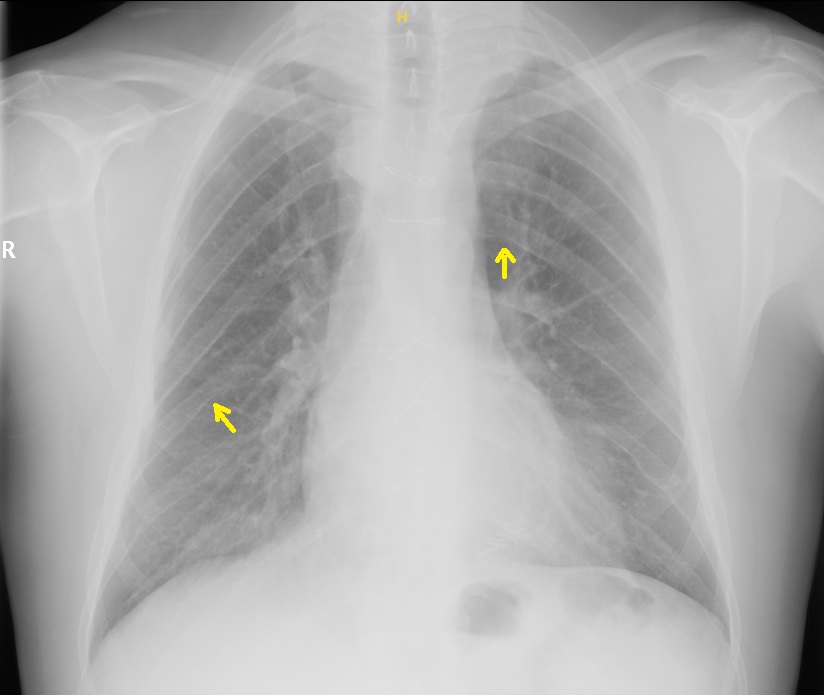
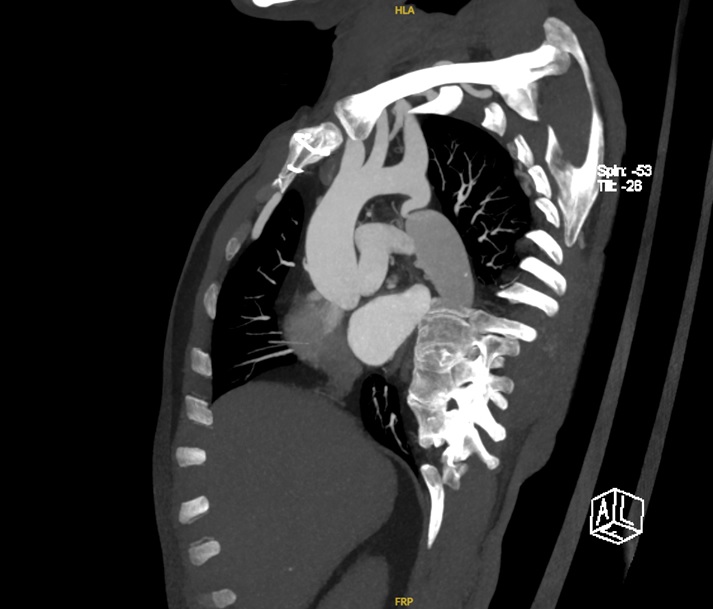
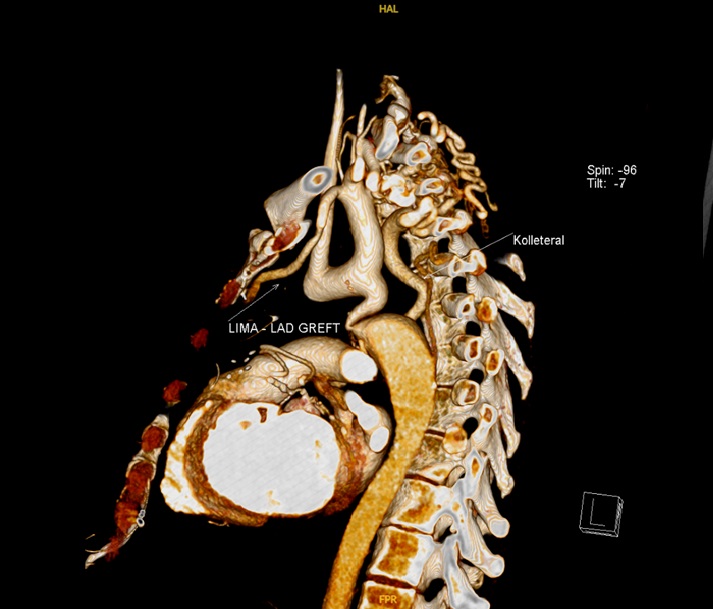
Embolization was planned for aneurysm, and during cerebral angiography, CoA was diagnosed. Chest X-ray demonstrated rib notching. Cardiac CT was performed in order to detect possible other congenital heart diseases and evaluate the CABG grafts. Coronary grafts were patent and post-ductal CoA was reported. His complete blood count, kidney and liver function test were normal. Echocardiography revealed normal LVEF (62%) with mild left ventricular hypertrophy.
Relevant Catheterization Findings
Increased gradient was established in echocardiographic evaluation. Covered stent implantation was planned and measured translesional gradient by angiography was peak to peak 30 mmHg. Aortographic images showed significant CoA (Video-1).
 Video1.mp4
Video1.mp4
Interventional Management
Procedural Step
Sheaths were inserted to the bilateral femoral arteries and left brachial artery. A pigtail catheter was placed proximally to the CoA via brachial artery and stenotic segment was passed with hydrophilic wire and Judkins R catheter. Amplatzer Stiff wire was replaced with hydophilic wire (Video-2). Recurrent step-by-step percutaneous transluminal angioplasty was performed with gradually increased sized balloons (Video-3). After successful balloon angioplasty, a covered stent (39 mm) was implanted in the stenotic segment (Video-4). Translesional gradient was decreased from 30 mmHg to 3 mmHg. Sheaths were displaced and femoral artery insertion site was closed with ProGlide vascular closure system. Further coil embolization for ACA aneurysm was scheculed and patient was discharged after 24 hours follow up in intensive care unit.
Video-2.mp4
Video-3.mp4
Video-4.mp4
Case Summary
Coarctation of aorta (CoA) is a rare anomaly and it usually presents with hypertension in young adults. This case shows that CoA may be overlooked if the physical examination was not performed carefully. CoA is an important clinical picture because it may cause atrial fibrillation, accelerated coronary artery disease. Berry aneurysms of the Willis circle may present in 10% of the CoA patients. CoA should be excluded in hypertensive patients with Berry aneurysm.CoA should be kept in mind in patients with claudication and normal peripheral arteries. CoA may be overlooked even in patients who underwent CABG surgery if coronary angiography was performed via transradial approach.