
Lots of interesting abstracts and cases were submitted for TCTAP 2022. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-086
Protected PCI for a CHIP Case
By Karnakar Rapolu
Presenter
Karnakar Rapolu
Authors
Karnakar Rapolu1
Affiliation
Apollo Health City, Hyderabad, India1,
View Study Report
TCTAP C-086
CORONARY - Complex and Higher Risk Procedures for Indicated Patients (CHIP)
Protected PCI for a CHIP Case
Karnakar Rapolu1
Apollo Health City, Hyderabad, India1,
Clinical Information
Patient initials or Identifier Number
RRV
Relevant Clinical History and Physical Exam
61 Years Old Gentle Man
Diabetic
Old Anterior wall MI
Primary PTCA was done and stented the Osteo-Proximal LAD in 2017
Now presented with Unstable angina and shortness of breath (SOB) Functional Class III
Diabetic
Old Anterior wall MI
Primary PTCA was done and stented the Osteo-Proximal LAD in 2017
Now presented with Unstable angina and shortness of breath (SOB) Functional Class III
Relevant Test Results Prior to Catheterization
ECG: Left Ventricular Hypertrophy. Poor R wave progression from v1 - v6ECHO: Dilated LV, RWMA in LAD territory, Severe LV Systolic Dysfunction.PET Viability: All territories were Viable.
Relevant Catheterization Findings
Angiogram Findings:
Distal LMCA Lesion. Double vessel disease (ISR in LAD and Ostio-ProximalLCX lesion.
Plan and Strategy:Patient developed Acute LV Failure post angiogram inthe CathlabStabilized with diuretics and inotropes.Surgeon denied CABG in view of severe LV dysfunction,recent LVF and poor targets.Planned for CHIP intervention with Impella support.(Protected PCI)DK crush Technique
 ANGIOGRAM 2.mp4
ANGIOGRAM 2.mp4
ANGIOGRAM.mp4
Distal LMCA Lesion. Double vessel disease (ISR in LAD and Ostio-ProximalLCX lesion.
Plan and Strategy:Patient developed Acute LV Failure post angiogram inthe CathlabStabilized with diuretics and inotropes.Surgeon denied CABG in view of severe LV dysfunction,recent LVF and poor targets.Planned for CHIP intervention with Impella support.(Protected PCI)DK crush Technique
Interventional Management
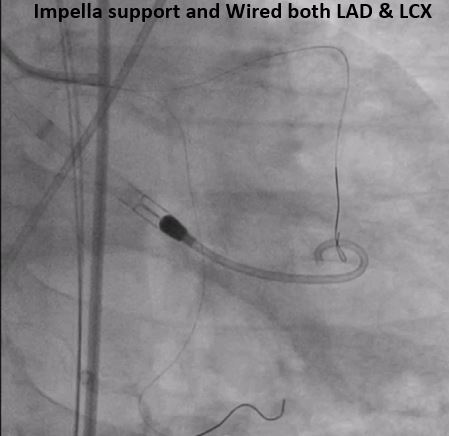
Procedural Step
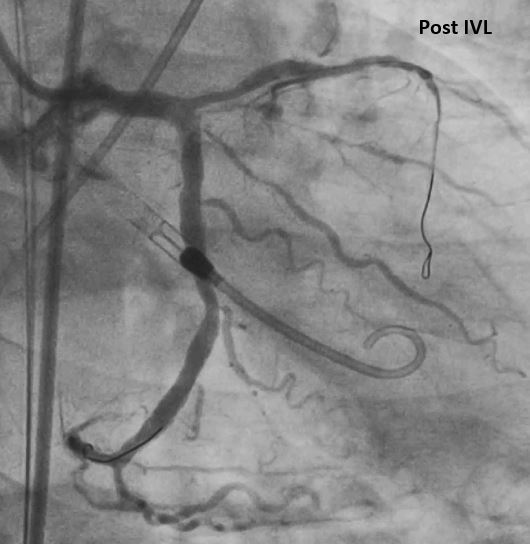
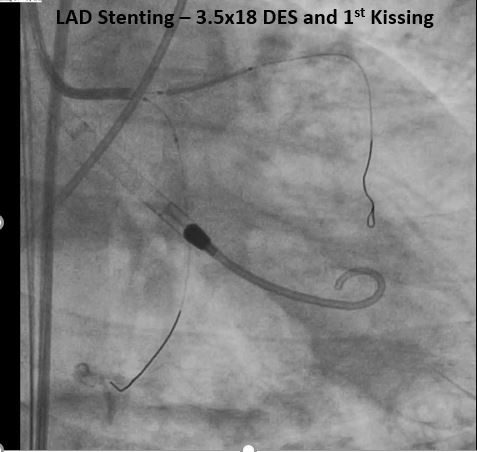
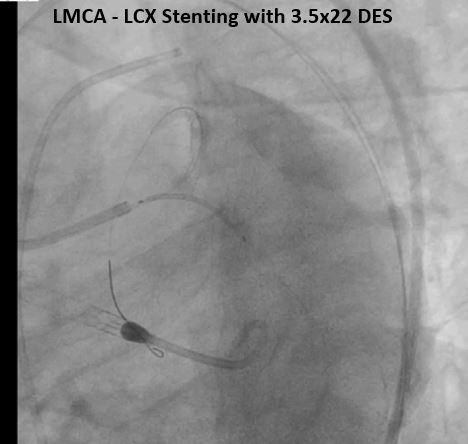
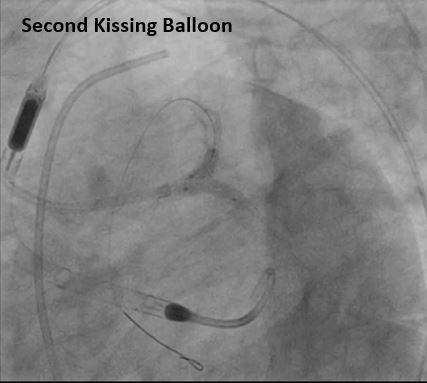
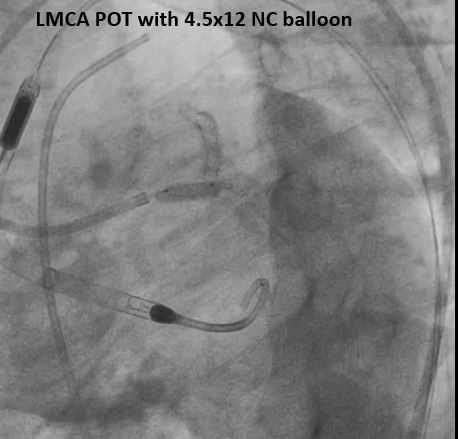
Placed Multipurpose catheter inmain pulmonary artery for hemodynamic monitoring. Punctured Left Femoral arteryunder ultrasound guidance with micro puncture set. Vascular closure device placed. 2.5 Impella was placed acrossaortic valve. LMCA engaged with 7F guidingcatheter. LAD and LCX wired with workhorseguidewires. Tried to cross OCT imagingcatheter but it could not able to cross the lesion because of severe calcium. Predilated the LAD lesion with2.5x12 NC balloon. Sequentially predilated the LCXlesion with 3.0x12 & 3.5x12 NC balloons. Then tried to cross OCT catheter again but could not cross as the lesion is calcified.The lesion was dilated with 3.5x10 scoring balloon. As the OCT catheter could not cross the lesion. IVL done with 3.5x12 IVL balloon bygiving 80 pulses. OCT catheter could not cross. Finally OCT catheter successfullycrossed with Guideliner support. OCT shown severe calcium withprotruding nodules in ostial LCX and distal left main. Dilated the LAD lesion with 3.0x12NC balloon, Then decided to go with DK crush technique. Ostio proximal LAD lesion Stented with 3.0x18DES at 18 ATM. Crushed the LAD stent with 3.0x12 NC balloon. Re-crossed and First Kissing Done. Stented LMCA to LCX with 3.5x22 DES. Second Kissing Done, Post dilated with 4.0x12 NC balloon. POT Done with 4.5x12 NC balloon. OCT shown good stent apposition and expansion. Final result shown TIMI 3 Flow. Impella Removed and Vessel closed with Pre-closure device.
Case Summary
In CHIP Interventions, Mechanical Circulatory SupportDevices are useful for Successful PCI when option of CABG is not available.Mechanical Circulatory Support Devices providesgood hemodynamic support in high-risk PCI.