
Lots of interesting abstracts and cases were submitted for TCTAP 2022. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-013
Successful Emergency PCI in a Case With Severely Angulated Left Anterior Descending Artery Using S-Shaped Wire
By Yi Xu, Dongdong Chen, Ning Bian, Jianyi Feng, Jinlong Wang, Shaorong Wu, Jun Guo, Zicheng Li
Presenter
Yi Xu
Authors
Yi Xu1, Dongdong Chen2, Ning Bian2, Jianyi Feng2, Jinlong Wang2, Shaorong Wu2, Jun Guo2, Zicheng Li2
Affiliation
The First Affiliated Hospital of Jinan University, China1, First Affiliated Hospital of Ji'Nan University, China2,
View Study Report
TCTAP C-013
CORONARY - Acute Coronary Syndromes (STEMI, NSTE-ACS)
Successful Emergency PCI in a Case With Severely Angulated Left Anterior Descending Artery Using S-Shaped Wire
Yi Xu1, Dongdong Chen2, Ning Bian2, Jianyi Feng2, Jinlong Wang2, Shaorong Wu2, Jun Guo2, Zicheng Li2
The First Affiliated Hospital of Jinan University, China1, First Affiliated Hospital of Ji'Nan University, China2,
Clinical Information
Patient initials or Identifier Number
ZLZ
Relevant Clinical History and Physical Exam
A 55-year-old woman with severe chest pain for 5 hours visited the emergency department of our hospital. The pain was squeezing and radiated to her left arm. She had a history of hypertension for 5 years and no other comorbidities. She presented diaphoretic and weakness with blood pressure of 165/101 mmHg, pulse 84 bpm, respiratory rate 21, and body temperature 36.1℃. Physical examination showed no significant findings.
Relevant Test Results Prior to Catheterization
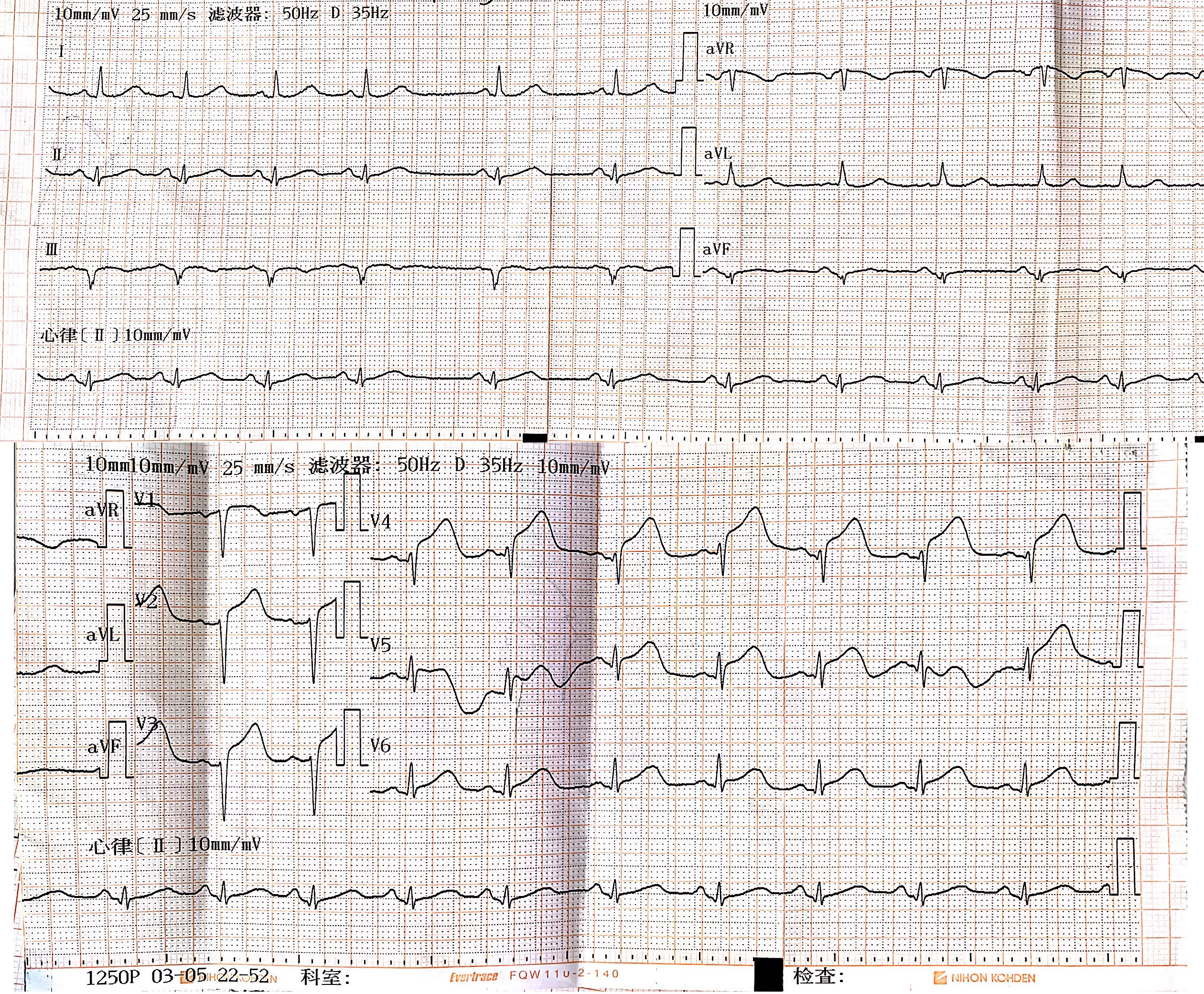
The electrocardiography showed sinus rhythm with elevation of J point and-segment on leads V1-V5. Laboratory tests came out with significantly raised high-sensitivity cardiac troponin-I level of 100 ng/ml. The patient was diagnosed with acute myocardial infarction (AMI) and was given a loading dose of aspirin 300 mg and ticagrelor 180 mg. She was immediately transferred to our catheter lab for emergency coronary angiography (CAG).
Relevant Catheterization Findings
The left anterior descending artery (LAD) was severely angulated and tortuous as it branched from the left main trunk. The LAD was completely occluded with TIMI 0 blood flow from its proximal part. The circumflex artery was also tortuous but there wasn't any significant stenosis. There was a 50% stenosis at middle right coronary artery (RCA), but there weren’t any signs of formation of collateral circulation at the distal part that supplies the left coronary artery system.
 Zhu_Li_Zhen_642642_43.avi
Zhu_Li_Zhen_642642_43.avi
Zhu_Li_Zhen_642642_57.avi
Zhu_Li_Zhen_642642_42.avi
Interventional Management
Procedural Step
The left coronary system was engaged with a 6F EBU 3.5 guiding catheter. A Runthrough wire was not able to pass through the angulated proximal LAD. Another attempt with Runthrough under Finecross microcatheter support also failed. A harder Sion wire also couldn’t pass through. After a few attempts, we took out the Sion wire and formed its tip into an “S” shape with 2 curves. The S-shaped wire was finally able to advance through the severely angulated vessel with careful adjusting and tip rotation. Another Runthrough wire was then exchanged. A dose of 8 mg intracoronary tirofiban was administered to prevent re-occlusion of the LAD. The lesion was pre-dilated with a 2.0*15 mm Emerge balloon at 12 atm. A Resolute Integrity 2.75*18 mm drug-eluting stent was deployed at the LAD lesion at 8 atm. The stent was post-dilated with a 2.75*8 mm NC Quantum balloon at 12-16 atm. Angiography re-evaluation showed that the stent was well deployed with TIMI 3 blood flow and no complications. The patient was then transferred to our cardiology department for further observation. The total procedural time was 84 minutes.
Zhu_Li_Zhen_642642_54.avi
Zhu_Li_Zhen_642642_33.avi
Zhu_Li_Zhen_642642_29.avi
Case Summary
We described a successful PCI for an AMI patient whose LAD was severely angulated. Intracoronary imaging techniques, though helpful, was not used here due to limited time. We used the “S-shaped wire” technique to advance through and treat the culprit vessel in time. The tip of the wire was formed and bent into an “S” shape with two curves. The bigger curve at bottom provided support while the smaller curve at the tip could slip into the angulated vessel under careful rotation. This technique can be considered a possible treatment strategy for these severely angulated vessels in emergency procedures and is worth further studying.