
Lots of interesting abstracts and cases were submitted for TCTAP 2022. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-100
Left Main Culotte Stenting as Bail-Out Strategy in Optical Coherence Tomography Catheter - Induced Ostial Circumflex Dissection
By Aninka Saboe, Achmad Fauzi Yahya
Presenter
Aninka Saboe
Authors
Aninka Saboe1, Achmad Fauzi Yahya2
Affiliation
Dr. Hasan Sadikin Central General Hospital, Padjadjaran University, Indonesia1, Dr. Hasan Sadikin Central General Hospital, Indonesia2,
View Study Report
TCTAP C-100
CORONARY - Complications
Left Main Culotte Stenting as Bail-Out Strategy in Optical Coherence Tomography Catheter - Induced Ostial Circumflex Dissection
Aninka Saboe1, Achmad Fauzi Yahya2
Dr. Hasan Sadikin Central General Hospital, Padjadjaran University, Indonesia1, Dr. Hasan Sadikin Central General Hospital, Indonesia2,
Clinical Information
Patient initials or Identifier Number
TS
Relevant Clinical History and Physical Exam
A 53-year-old man was planned for staged PCI to distal LCx. He had a history of primary PCI, underwent stent implantation at the ostial LAD six months ago. Cardiovascular risk factors were hypertension and smoker. His vital sign and physical examinations were within normal limits.
Relevant Test Results Prior to Catheterization
An echocardiogram revealed a mid-range ejection fraction of 41% and regional wall motions abnormalities (hypokinetic at anteroseptal and inferolateral wall).
Relevant Catheterization Findings
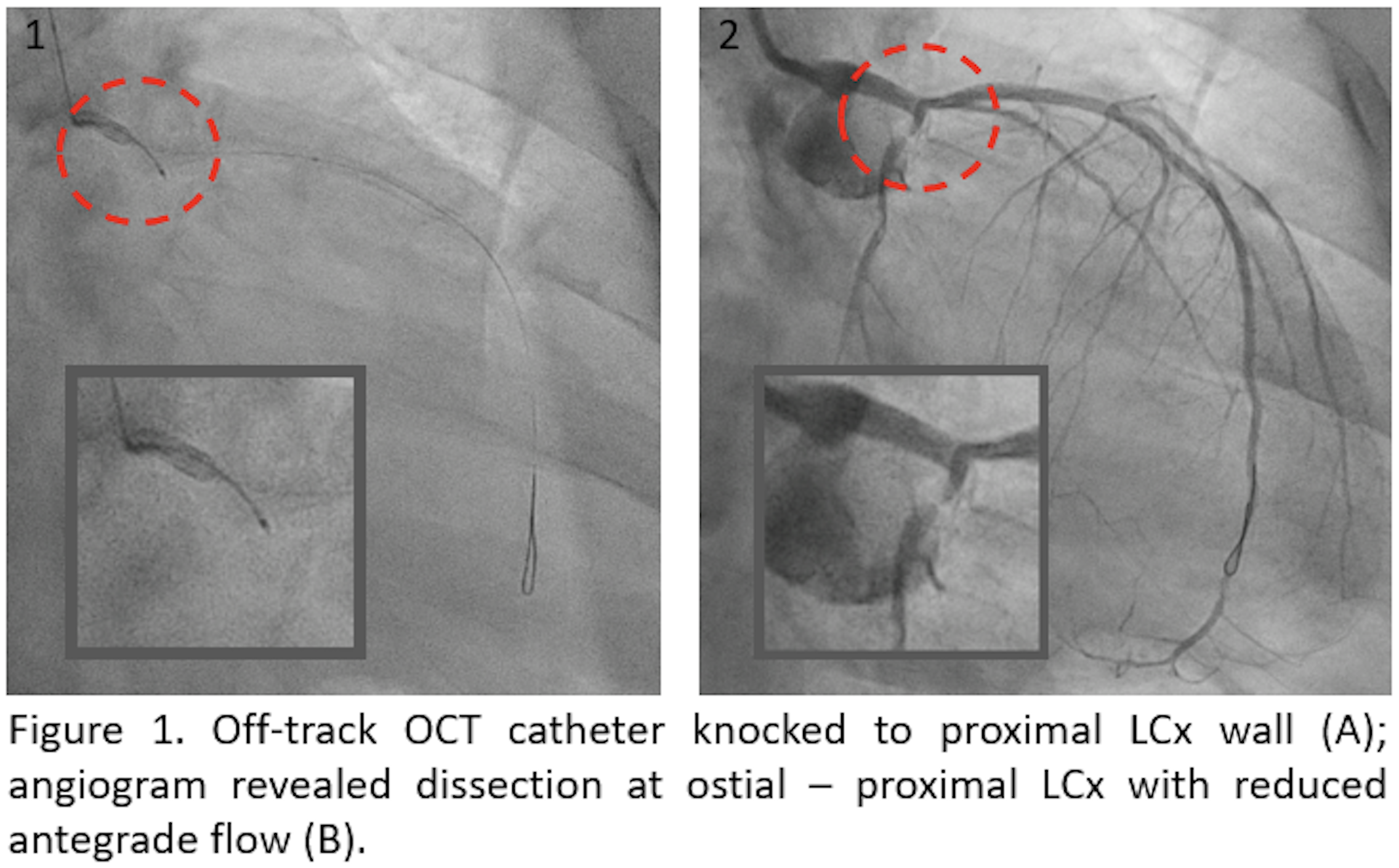
Coronary angiogram revealed mild to moderate stenosis at distal Left Main (LM). Stent at proximal LAD was patent with moderate stenosis at ostial LAD. There was a moderate stenosis at ostial LCx and significant stenosis at distal LCx. CTO RCA was visualized with collateral from LCx. Hence, we proceed with PCI to LCx. OCT study to LAD was performed before PCI LCx, but there was difficulty in delivering the catheter and it was displaced, knocked into the ostial LCx (Figure 1A).
 Fluoroscopy-16-16.mov
Fluoroscopy-16-16.mov
Interventional Management
Procedural Step
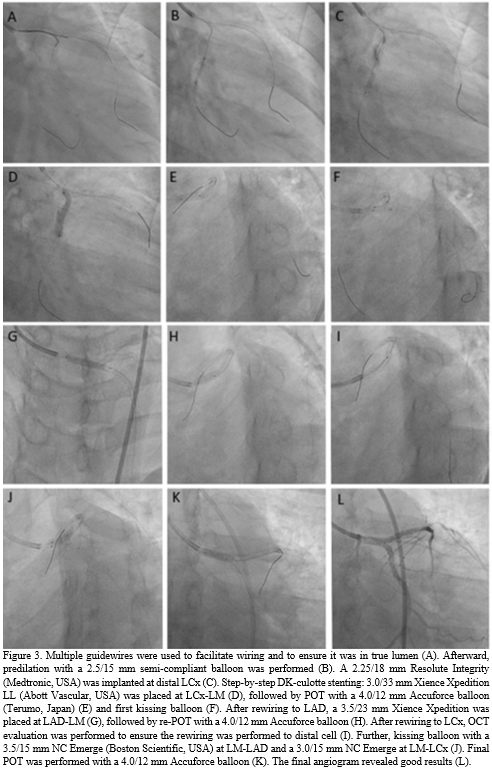
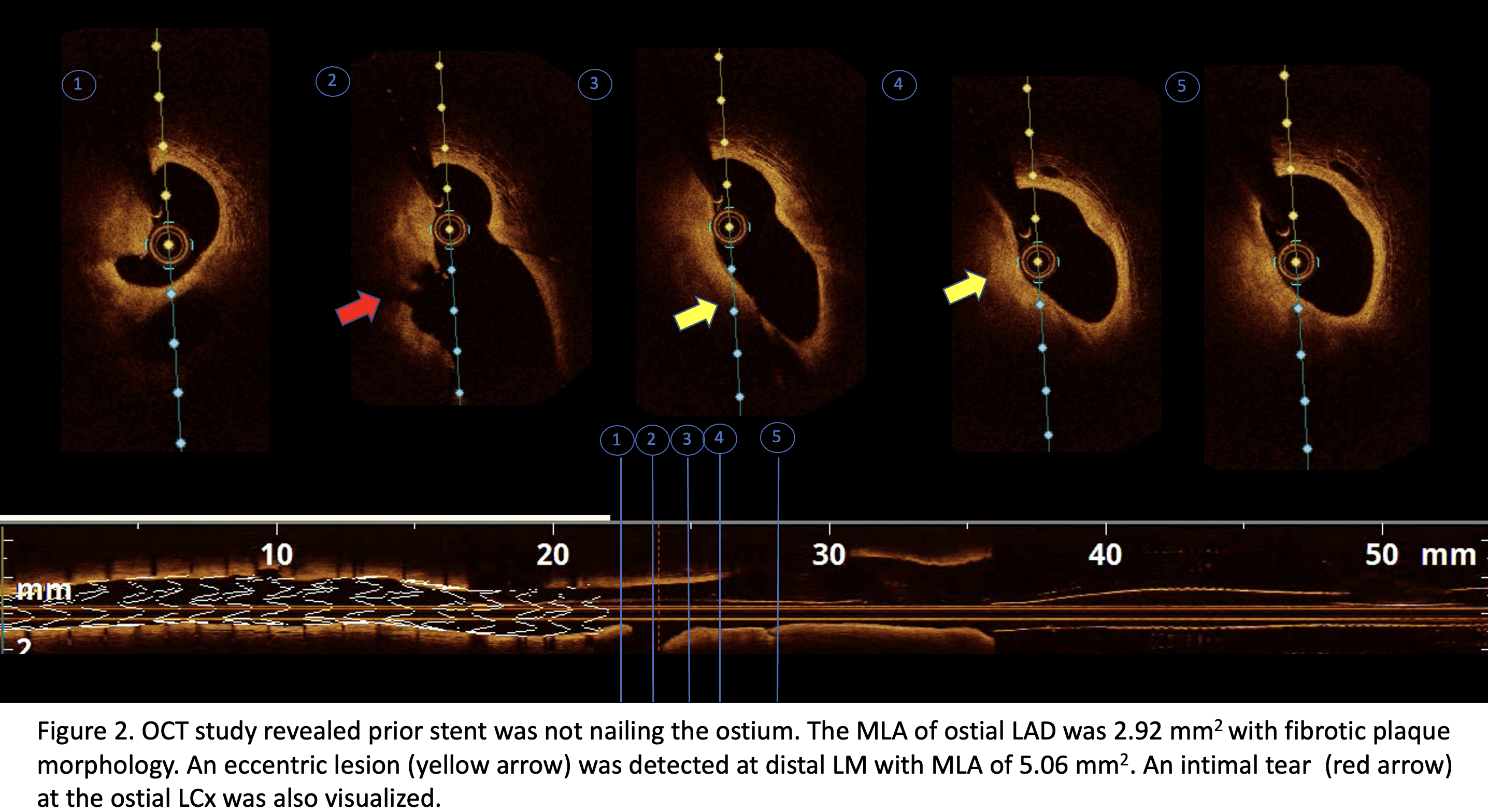
The guiding catheter was repositioned and after a more co-axial engagement, the OCT catheter was subsequently successfully advanced to distal LAD. The OCT run revealed fibrotic plaque at ostial LAD with MLA of 2.92 mm2 and eccentric lesion at distal LM with MLA of 5.06 mm2. An intimal tear at the ostial LCx was also visualized (Figure 2). Careful contrast injection revealed dissection at the ostial-proximal part of LCx with the reduced antegrade flow and compromised collateral flow to RCA (Figure 1B). The patient was experiencing chest pain with ECG that revealed ST elevation at the inferior lead.
Case Summary
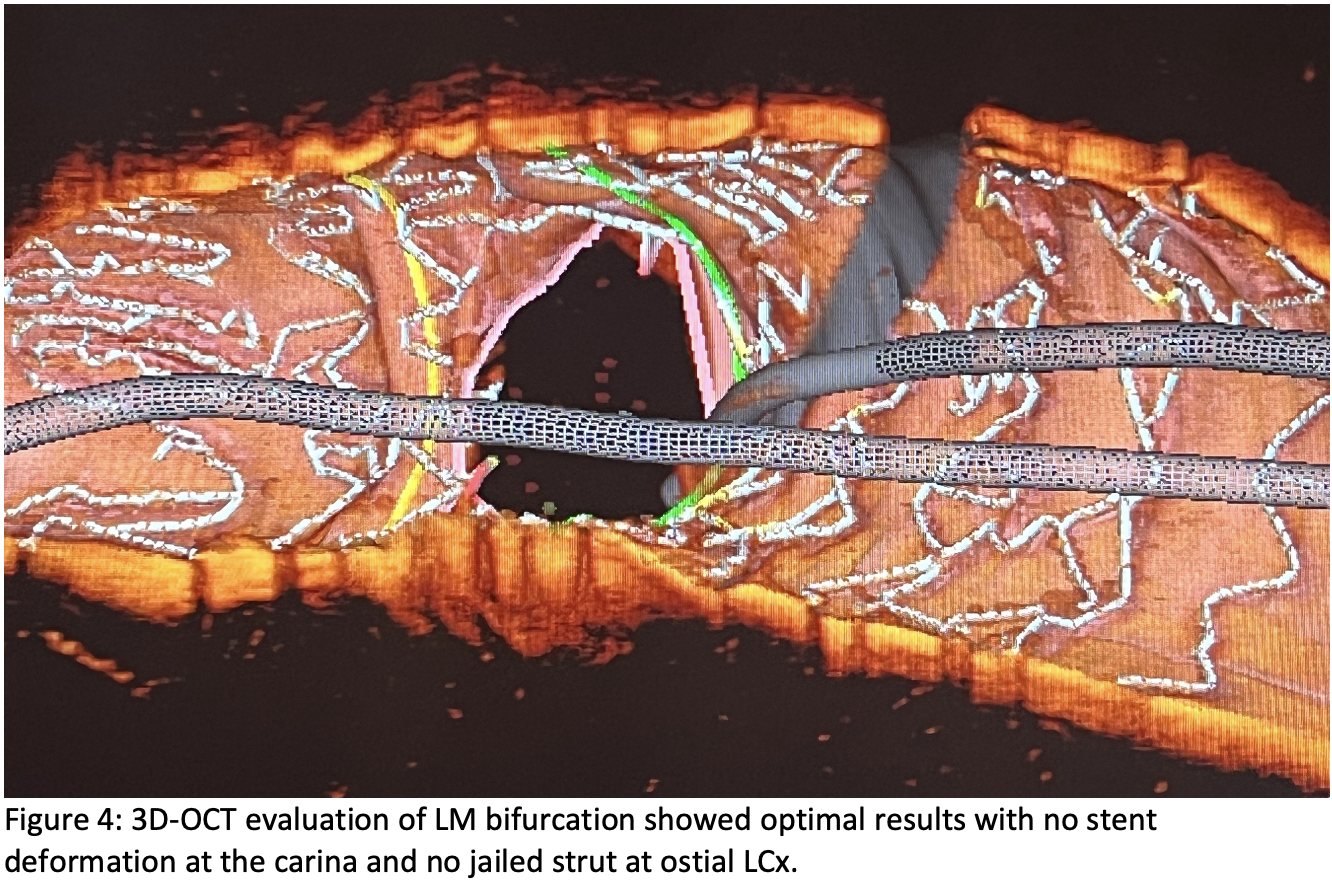
Despite its benefit, complications may be associated with the use of OCT. According to our knowledge, this is the first case describing ‘off-track’- OCT catheter–induced coronary dissection in LM bifurcation. This may be associated with the eccentric distal LM lesion creating a complex intraluminal route for the OCT catheter delivery. DK-culotte stenting is a feasible technique in managing complications as ostial LCx dissection in LM bifurcation lesion.