
Lots of interesting abstracts and cases were submitted for TCTAP 2022. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-040
High Risk PCI in a Patient With Triple Vessel Disease and Left Main Lesion: How to Overcome Challenges to Rewire the Side Branch by Using Guide Extension Catheter
By Nay Thu Win, Ting Yuen Beh, Kumara Gurupparan Ganesan
Presenter
Nay Thu Win
Authors
Nay Thu Win1, Ting Yuen Beh2, Kumara Gurupparan Ganesan2
Affiliation
Royal Free London, United Kingdom1, National Heart Institute, Malaysia2,
View Study Report
TCTAP C-040
CORONARY - Bifurcation/Left Main Diseases and Intervention
High Risk PCI in a Patient With Triple Vessel Disease and Left Main Lesion: How to Overcome Challenges to Rewire the Side Branch by Using Guide Extension Catheter
Nay Thu Win1, Ting Yuen Beh2, Kumara Gurupparan Ganesan2
Royal Free London, United Kingdom1, National Heart Institute, Malaysia2,
Clinical Information
Patient initials or Identifier Number
sbs
Relevant Clinical History and Physical Exam
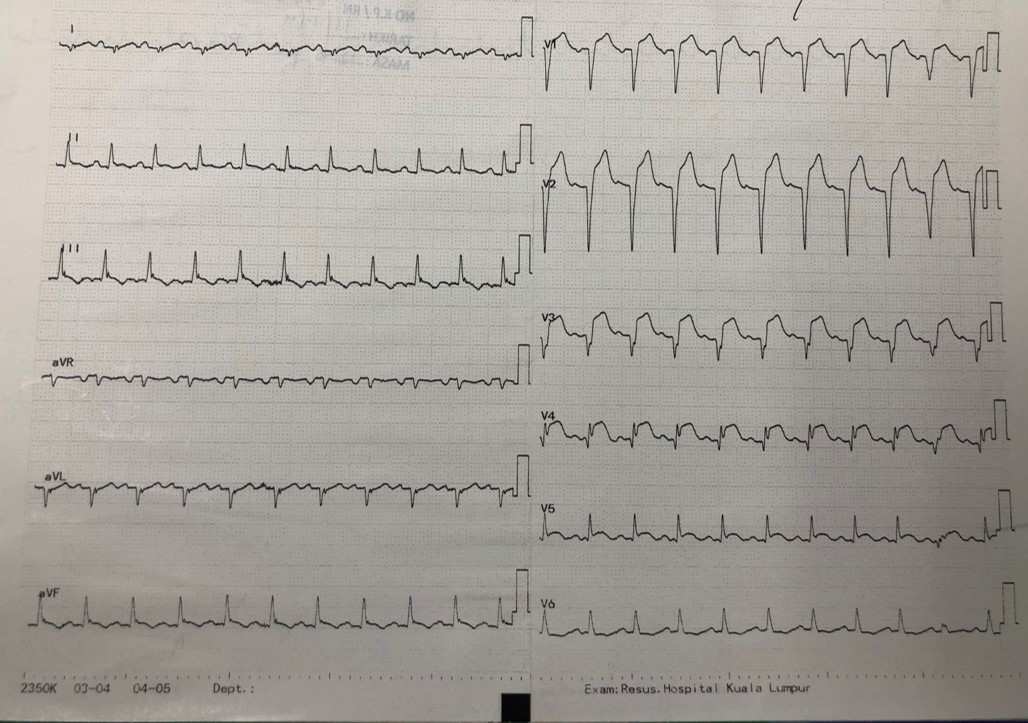
A 35 years old male patient, who is a smoker, presented with left sided chest pain associated with profuse sweating and palpitation to a non-PCI capable center. ECG showed ST elevation at V1 to V6 , Lead II and aVL with T inversion at II, III, aVF. Hence, he was diagnosed as extensive anterolateral STEMI and aspirin 300 mg and clopidogrel 300 mg was given stat, then referred to our center for primary PCI.
Relevant Test Results Prior to Catheterization
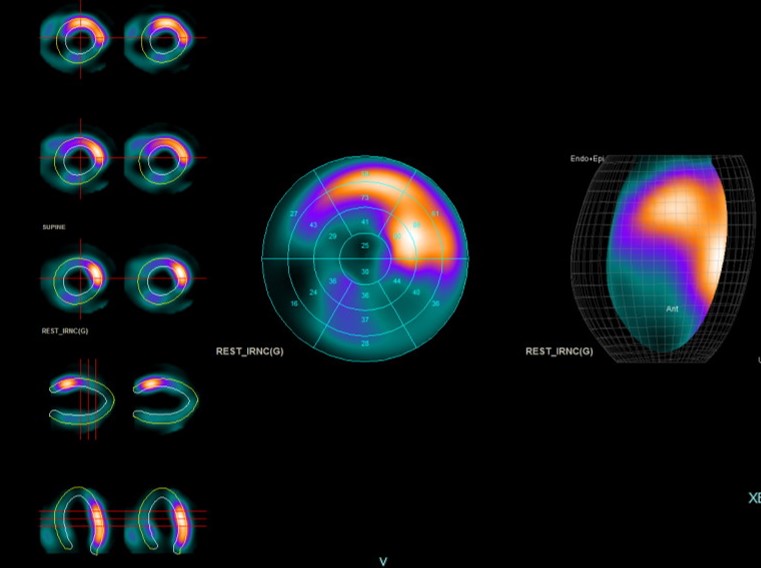
Blood investigations showed raised cardiac troponin andnormal renal function. HBA1c was normal. Technetium myocardial perfusion scan revealed there was infarcted myocardial segment in the distal LAD artery territory and distal RCA territory. The other segment showed normal viable myocardium with left ventricular ejection fraction of 54%.
Relevant Catheterization Findings
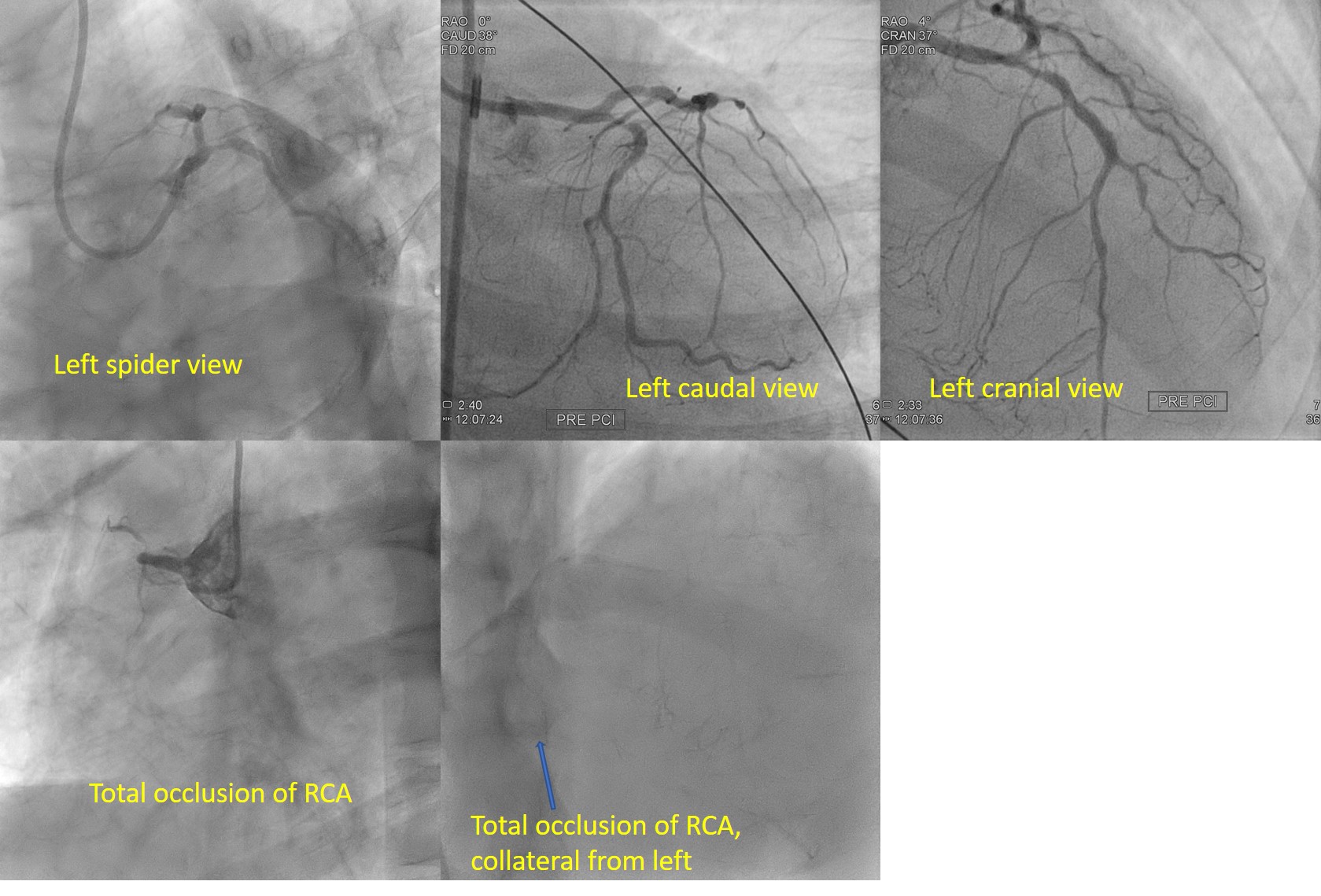
Coronary angiogram showed severe disease at distal left main, severe disease from ostial to proximal LAD, severe disease at LCX and total occlusion at right coronary artery. He was counselled for urgent coronary artery bypass graft surgery. Cardiothoracis team decided that he was not a good candidate for CABG in view of poor ejection fraction. Therefore, he was explained about the options of high risk PCI to LM, LAD and LCX. He understood clearly and keen to proceed for high risk PCI.
Interventional Management
Procedural Step
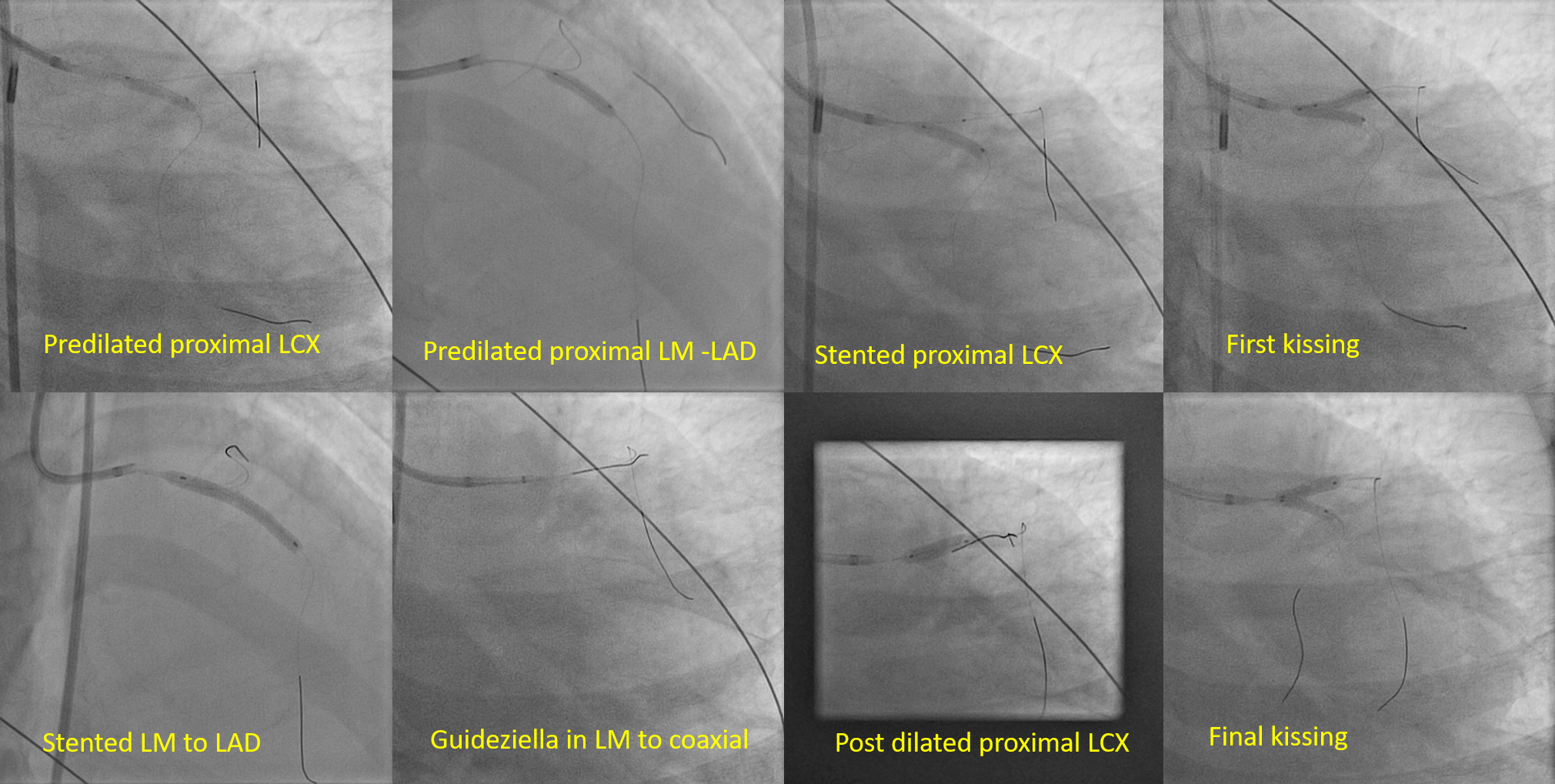
Right femoral approach with 7F sheath and EBU3.5/7F to left was used.IABP 34 cc was inserted via left femoral. Runthrough floppy to LAD and Sion-Blue to LCX.LCX waspredilated with NC SCOREFLEX 2.5 x 15mm at 14 ATM. Then LAD was predilated with NC SCOREFLEX 2.5x15 mm followed by NCSCOREFLEX 3.5x15mmsequentially. Left Circumflex Artery was stented with XIENCE ALPINE 3.0 x 15mmat 12 ATM while keeping NC Sapphire 3.5x15 mm balloon in LAD,subsequently stentin LCX was crushed with non-compliant balloon in LAD. LCXwas rewired with a newwire followed by First kissing performed with stentballoon 3.0x15mm in LeftCircumflex Artery and NC SAPPHIRE 3.5/15mm LAD at 12ATM. LAD was stented withXIENCE ALPINE 3.5x33mm. LCX was rewired with SIONBLUE aiming at proximal stentstrut and jail wire was removed. POT to LeftAnterior Descending with NCSAPPHIRE 3.5 x 15mm at high pressure 22 ATM. Wetried to deliver the balloon toLCX in order to do 2nd kissing. There was difficulty to insert balloon duesharp angulation. IVUS was used to confirm the wire location and stentapposition, which showed well apposed stent at LM and LAD. Guideziella was used to coaxial with left main to facilitate balloon delivery to LCX. Wesuccessfully delivered a semicompliant balloon 2.0 x 12mm to postdilate ostialof LCX. After that, second kissing wasdone with NC EMERGE MONORAIL 3.0x12mm with Left Circumflex Artery and NCSCOREFLEX 3.5 x15mm at 12ATM. TIMI III flow achieved without complication.
 stent lcx.mpg
stent lcx.mpg
final lad.mpg
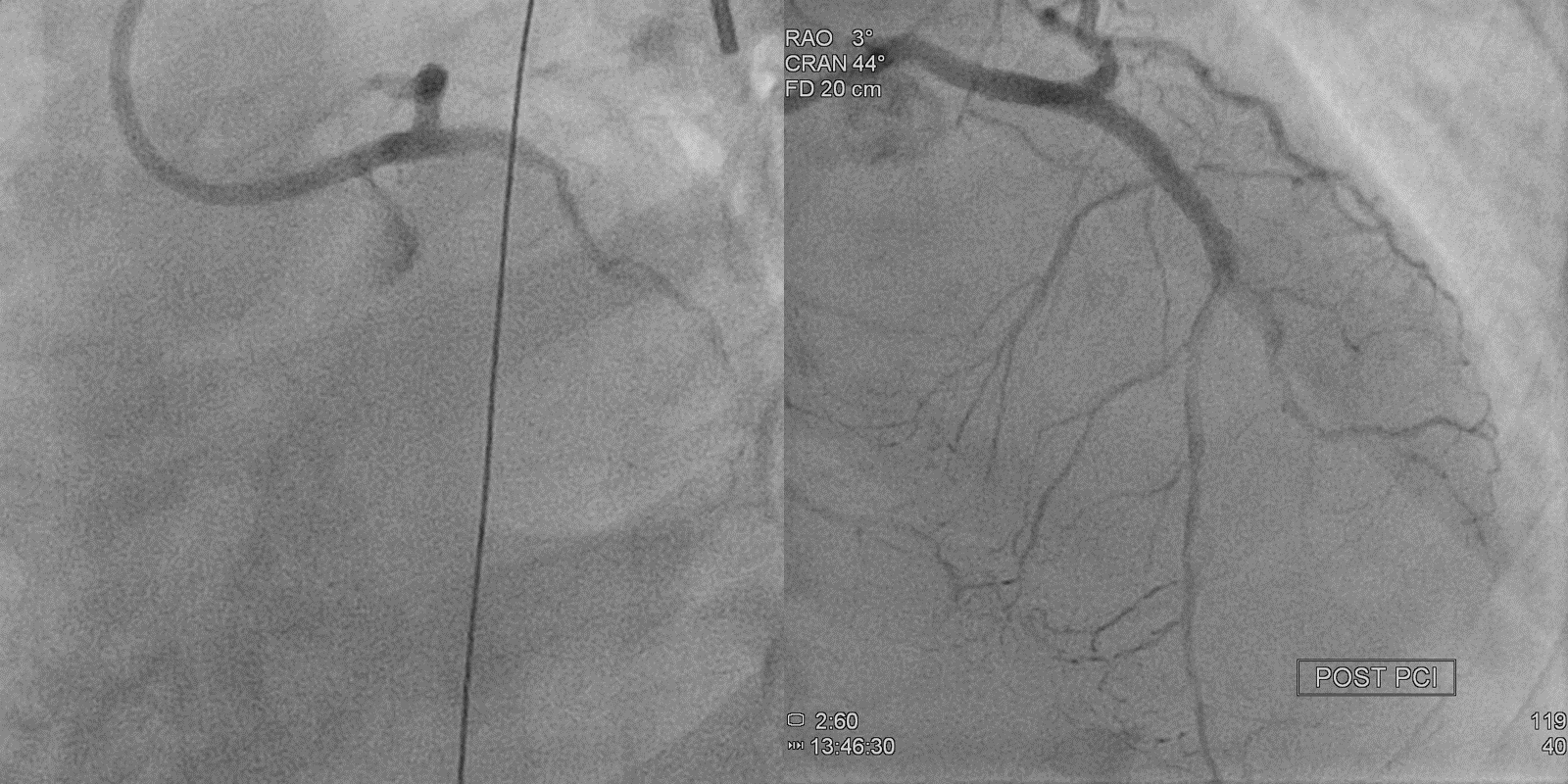
final result caud.mpg
Case Summary
Patient was successfully done high risk PCI to Left man, LAD and LCX by using two stents strategy: DK crush technique. Proximal optimisation technique is crucial to achieve the side branch rewiring and stent optimisation. Guide extension catheter Guideziella was used to facilitate rewiring to the side branch which improved coaxiality and stability of guiding catheter. Intravascular imaging supported the stent optimisation in left main and confirmation of wire in stent strut while rewiring.