
Lots of interesting abstracts and cases were submitted for TCTAP 2022. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-021
Hiccup After Hiccup - A Calcified CHIP Case With Multiple Challenges
By Fathima Aaysha Cader, Saidur Rahman Khan
Presenter
F. Aaysha Cader
Authors
Fathima Aaysha Cader1, Saidur Rahman Khan1
Affiliation
Ibrahim Cardiac Hospital & Research Institute, Bangladesh1,
View Study Report
TCTAP C-021
CORONARY - Adjunctive Procedures (Thrombectomy, Atherectomy, Special Balloons)
Hiccup After Hiccup - A Calcified CHIP Case With Multiple Challenges
Fathima Aaysha Cader1, Saidur Rahman Khan1
Ibrahim Cardiac Hospital & Research Institute, Bangladesh1,
Clinical Information
Patient initials or Identifier Number
CC
Relevant Clinical History and Physical Exam
A 74 year old Bangladeshi male presented with Canadian Cardiovascular Society (CCS) Class III-IV angina for 3-4 weeks, despite optimal medical therapy. He was diabetic, hypertensive and dyslipidaemic. Examination was unremarkable.
Relevant Test Results Prior to Catheterization
ECG showed poor progression of R wave V1-V4. Echo showed a left ventricular ejection fraction of ~55% with inferior wall hypokinesia.
Relevant Catheterization Findings
Coronary angiography showed diffusely calcified LAD with 70% proximal stenosis and long-segment mid part disease of 90% stenosis. Principal OM has 80% proximal part stenosis. A dominant calcified RCA has 95-99% stenosis in its mid part with TIMI 1-2 flow and diffusely diseased PDA.
 CAG 1.avi
CAG 1.avi
CAG 2.avi
CAG 4.avi
Interventional Management
Procedural Step
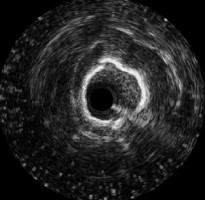
Using JL 3.5 6 F guide, the LAD was wired. IVUS showed napkin ring calcification of LAD. Workhorse wire was exchanged for Rota wire through microcatheter and 3 runs of rotational atherectomy with 1.25 mm burr at 160,000 rpm was done, followed by further lesion preparation with 2.5x15 mm NC balloon at 16 ATM. LAD was stented with 2.75x38mm drug eluting stent (DES). The OM was then wired and stented directly with2.5x8 mm DES. The RCA was engaged with the same guide. The lesion was crossed with 1.25 mm balloon support and predilated. IVUS showed diffuse calcification. Further sequential predilatation was done with 2.0x8 and2.5x15 mm NC balloons and 2.5x10 mm scoring balloon up to 16 ATM, through a5-in-6 French guide extension catheter. A DES was then passed through the guide extension, which would not cross and was stuck. On retrieval of the entire system, the stent was seen to be fractured at the point of entry through the guide extension catheter. A fresh catheter was taken and the RCA was stented with 3.0x30 mm DES at 12 ATM, with good angiographic result.
LAD Rota.avi
RCA scoring balloon and guidezilla.avi
RCA stent and guidezilla.avi

Case Summary
This case demonstrates important techniques for treating calcified lesions in resource-constrained environments as well as bailout strategies. In addition to root ablation, active and passive support, including guide extension, alpha loops, deep intubation may be needed for safe passage of balloons for adequate lesion preparation and stent deployment. Imaging guidance is key at every step. Guide extension catheters are not without complications – stent fracture may occur especially in calcified coronaries and one needs to be aware especially when crossing stents across calcified lesions through them.