
Lots of interesting abstracts and cases were submitted for TCTAP 2022. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-067
“Salvaging Heart and Saving Limb “: Thanks to Gruentzig and Dotter!
By Nagendra Boopathy Senguttuvan, Santhosh Kumar Periyasamy, Manokar Panchanatham, Thoddi Ramamurthy Muralidharan, Vinod Kumar Balakrishnan, Ramesh Sankaran, Preetam Krishnamurthy
Presenter
Santhosh Kumar Periyasamy
Authors
Nagendra Boopathy Senguttuvan1, Santhosh Kumar Periyasamy2, Manokar Panchanatham1, Thoddi Ramamurthy Muralidharan1, Vinod Kumar Balakrishnan1, Ramesh Sankaran3, Preetam Krishnamurthy1
Affiliation
Sri Ramachandra Institute of Higher Education and Research, India1, Sri Ramachandra Medical Center, India2, Sribalaji Medical College, India3,
View Study Report
TCTAP C-067
CORONARY - Complex and Higher Risk Procedures for Indicated Patients (CHIP)
“Salvaging Heart and Saving Limb “: Thanks to Gruentzig and Dotter!
Nagendra Boopathy Senguttuvan1, Santhosh Kumar Periyasamy2, Manokar Panchanatham1, Thoddi Ramamurthy Muralidharan1, Vinod Kumar Balakrishnan1, Ramesh Sankaran3, Preetam Krishnamurthy1
Sri Ramachandra Institute of Higher Education and Research, India1, Sri Ramachandra Medical Center, India2, Sribalaji Medical College, India3,
Clinical Information
Patient initials or Identifier Number
A
Relevant Clinical History and Physical Exam
79 years old male initially admitted elsewhere for planned peripheral angioplasty followed by right great toe amputation , developed in-hospital ACS -NSTEMI .CAG done revealed severe calcific triple vessel disease .Later in our hospital , patient was advised by pass surgery as the first option considering his co-morbids ( DM/PVD ) , however patient opted for high-risk PCI. O/E : VITALS : HR- 76/min BP -110/70 mm/hg CVS - S1S2 + RS - B/L AE +
Relevant Test Results Prior to Catheterization
LAB INVESIGATIONSHb- 12.5 gm /dl, TC- 11000, BUN – 18 mg, S. Creatinine - 0.7mg2D TTE- Regional wall motion abnormality noted in entire inferolateral, basal and mid inferoseptum, apical anterior and LV apex. Mild LV systolic dysfunction (EF-42%) noted.ECG – Normal sinus rhythm, no significant ST-T changes
Relevant Catheterization Findings
Interventional Management
Procedural Step
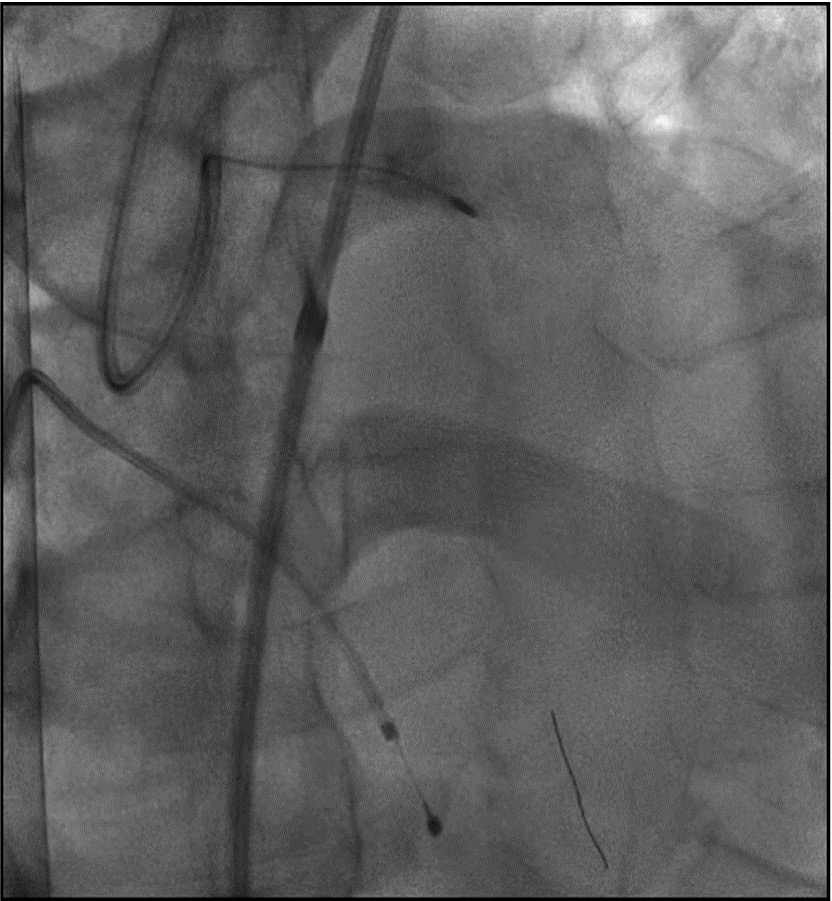
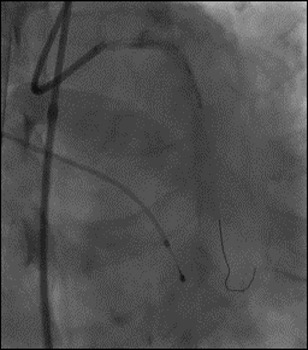
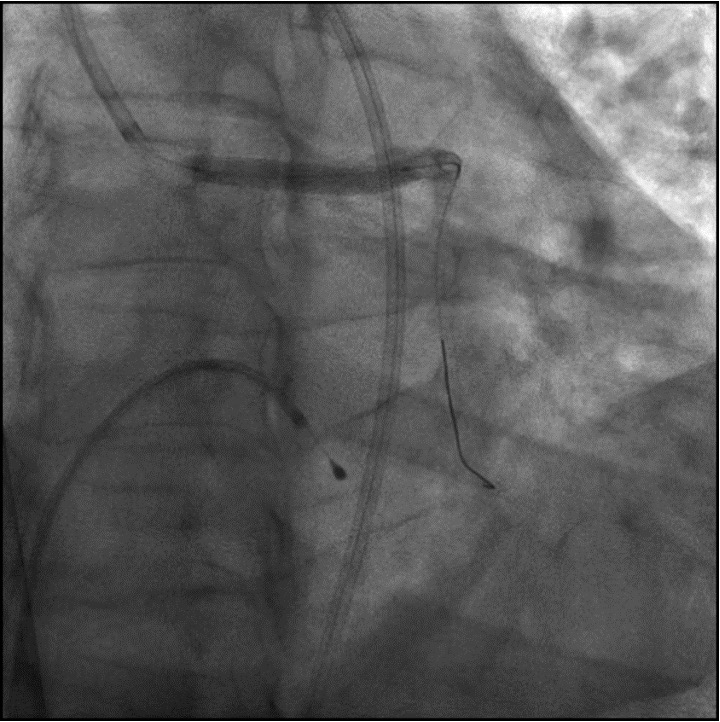
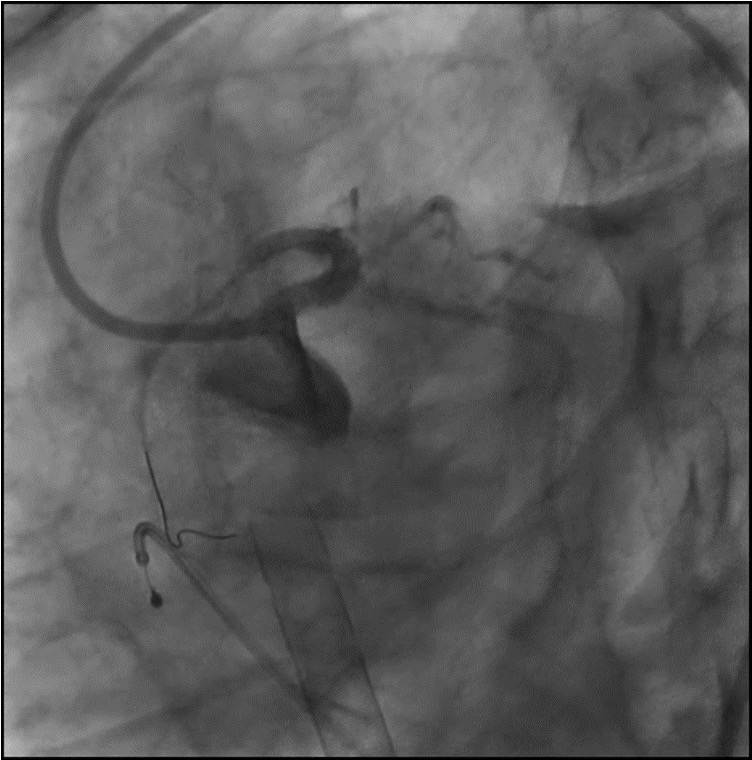
Both femoral access was taken and left femoral access was used for ECMO support. Initially with the support OF MICROCATHETER runthrough wire was used to cross the lesion in LAD. After failed attempt ROTA wire crossed the lesion and rotablation was tried with 1.5 & 1.25 ROTA BURR in LAD without much success. Rotablation in RI & LCX was done successfully using 1.25 BURR. LAD vessel bed prepared prepared for stenting using 2.0X10 mm NC balloon. Followed by predilatation using 2.5X6 mm NC balloon. Finally using 2.5X10 mm super hight pressure balloon predilatation done. POBA to LCX & RI done using 3.0X15mm cutting balloon .During pre dilatation balloon ruptured, patient developed hypotension Put on 100% ECMO support, which was later weaned to 50% and continue with the procedure.Left main to proximal LAD stenting was done using 3.5X26 mm DES Followed by post dilatation with 3.5X6 mm NC balloon, 4.0X6 mm NC balloon and finally with 4.5X6mm NC balloon.

 16.mp4
16.mp4
33.mp4
70.mp4
ECMO was decanulated on the table .Hemostasis achieved with the help of perclosure for 18 F arterial access and figure of 8 suture for 23F venous access. Balloon angioplasty of proximal & distal anterior tibial artery using 3.0X 80mm balloon. One week after the procedure he underwent amputation of great right toe successfully
Patient is doing well at 6 months follow-up.
Case Summary
MCS ( Impella, ECMO) protected PCI is very useful in high risk patients. Keeping it simple from the beginning of the case would have avoided stent dislodgement.IVL/Laser is an alternative atherectomy that could be used in such situations. Combined inter-disciplinary approach saves life and limb keeping the patient ambulatory