
Lots of interesting abstracts and cases were submitted for TCTAP 2022. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-063
Salvage for Long-tract False Lumen via IVUS Guidance in CTO Lesion
By Cheng-Han Lee, Yi-Jia Su
Presenter
Yi-Jia Su
Authors
Cheng-Han Lee1, Yi-Jia Su2
Affiliation
Tainan Municipal Hospital, Taiwan1, National Cheng Kung University Hospital, Taiwan2,
View Study Report
TCTAP C-063
CORONARY - Chronic Total Occlusion
Salvage for Long-tract False Lumen via IVUS Guidance in CTO Lesion
Cheng-Han Lee1, Yi-Jia Su2
Tainan Municipal Hospital, Taiwan1, National Cheng Kung University Hospital, Taiwan2,
Clinical Information
Patient initials or Identifier Number
12867319
Relevant Clinical History and Physical Exam
This 47-year-old man was a smoker with history of left tongue SCC, pT1N0M0G1R0, s/p surgery in 2021/06. His activity of daily living was independent. The patient mentioned an event of mild chest pain at around one year ago, with spontaneous symptom relieved. Also, mild dyspnea on exertion was noted in recent one year(still able to do laboring work), without obvious progression.
Relevant Test Results Prior to Catheterization
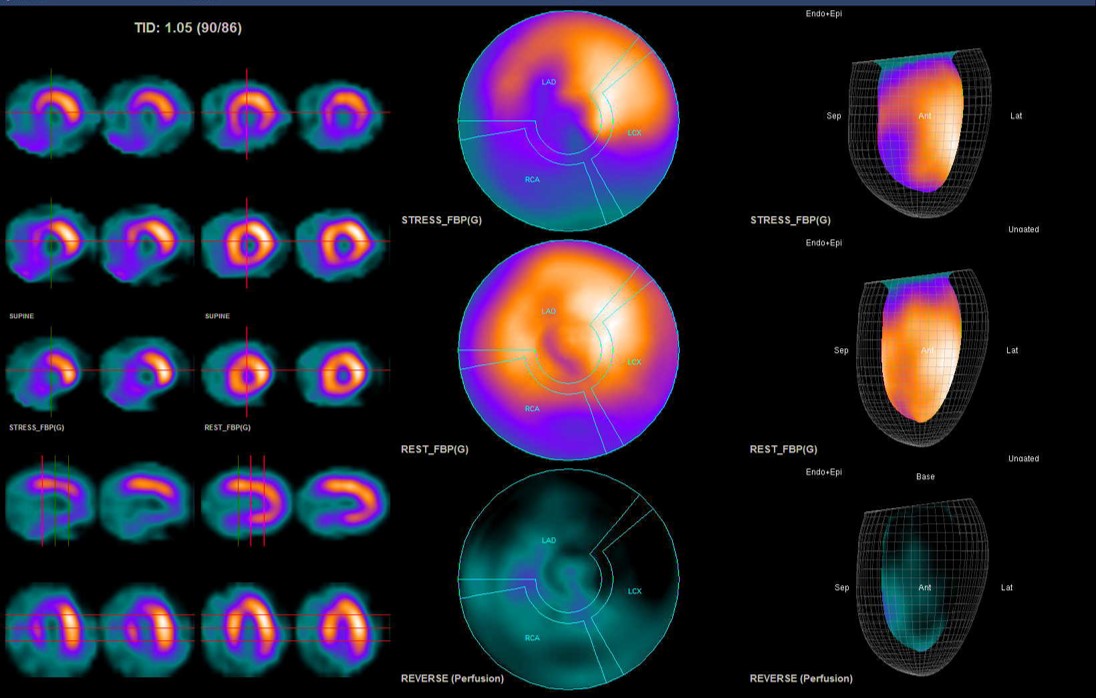
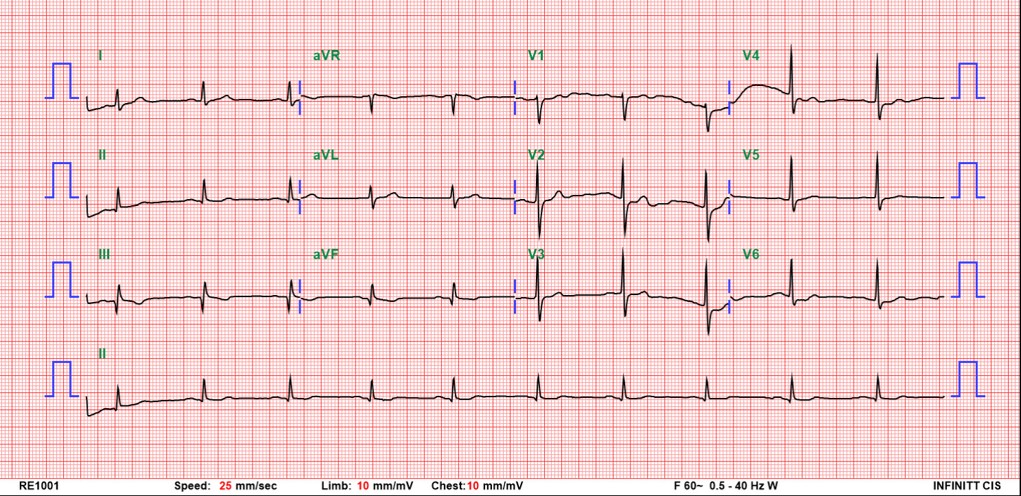
During pre-operation survey for tongue cancer 6 months ago, ECG showed T wave inversion and Q wave in lead II, III,aVF, suspect old MI. SPECT Dipyridamole stress test on 2021/06/08 showed severe stress-induced ischemia in the apical-to-basal inferior, basal inferolateral and mid-to-basal inferoseptal segments. Heart echo showed LVEF 75.8%.
Relevant Catheterization Findings
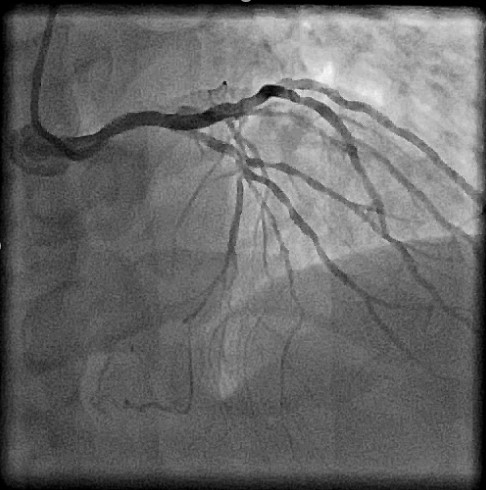
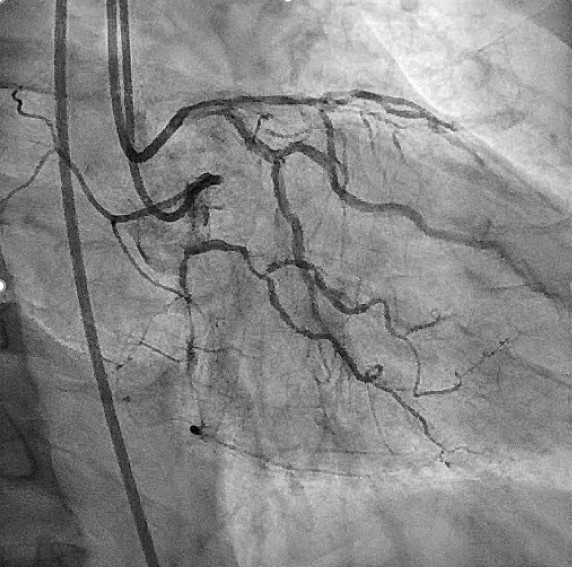
Percutaneous coronary angiography on 20201/06/30 found coronary artery disease (CAD) / 2-V-D, with chronic total occlusion over LAD-M to LAD-D and RCA-M to RCA-D, s/p bare metal stent (BMS) x1 to RCA-M and BMS x1 to RCA-D

Interventional Management
Procedural Step
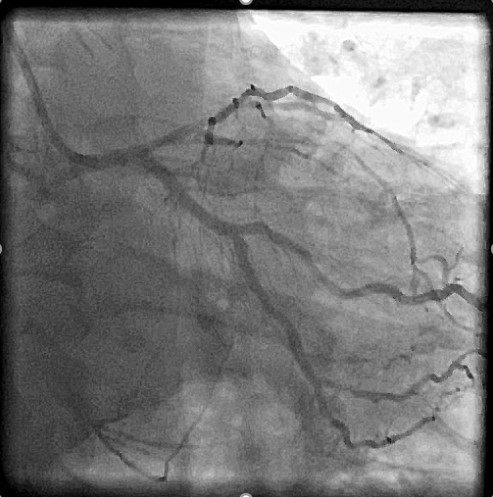
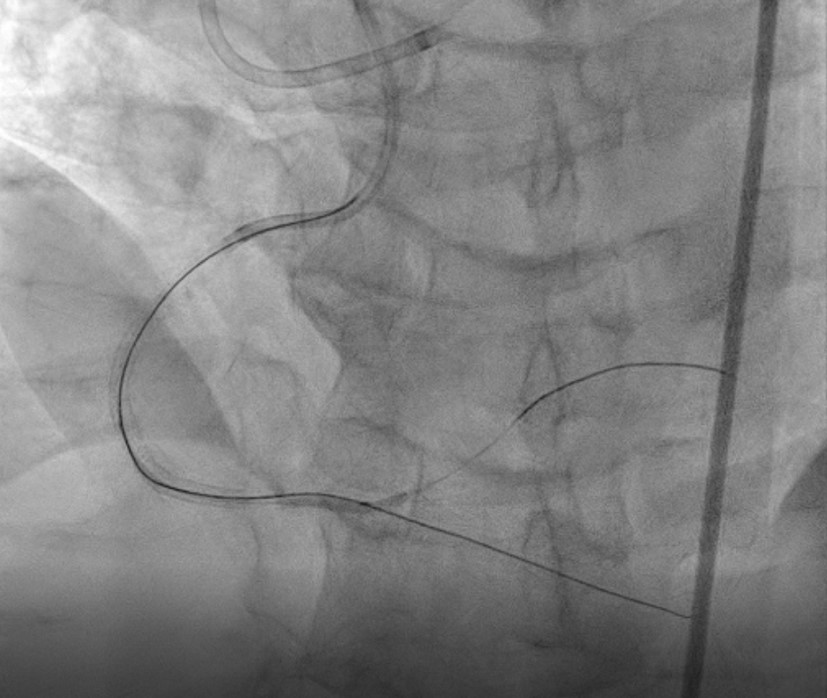
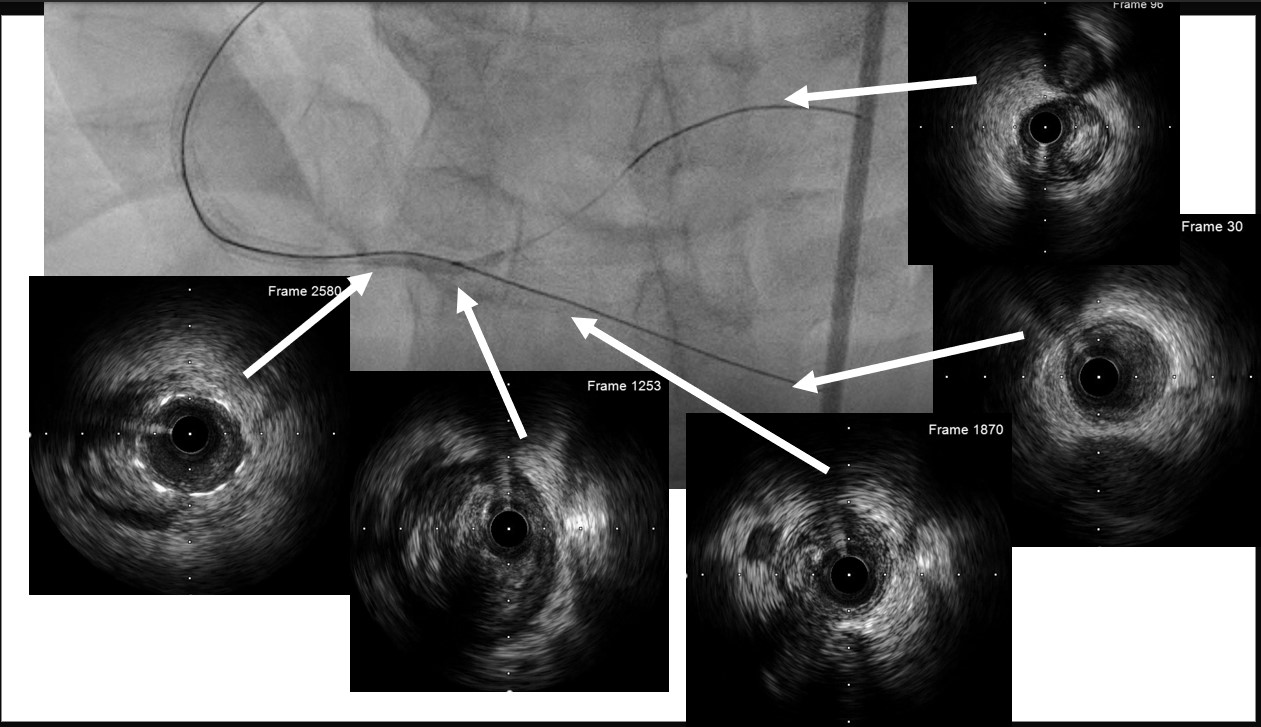
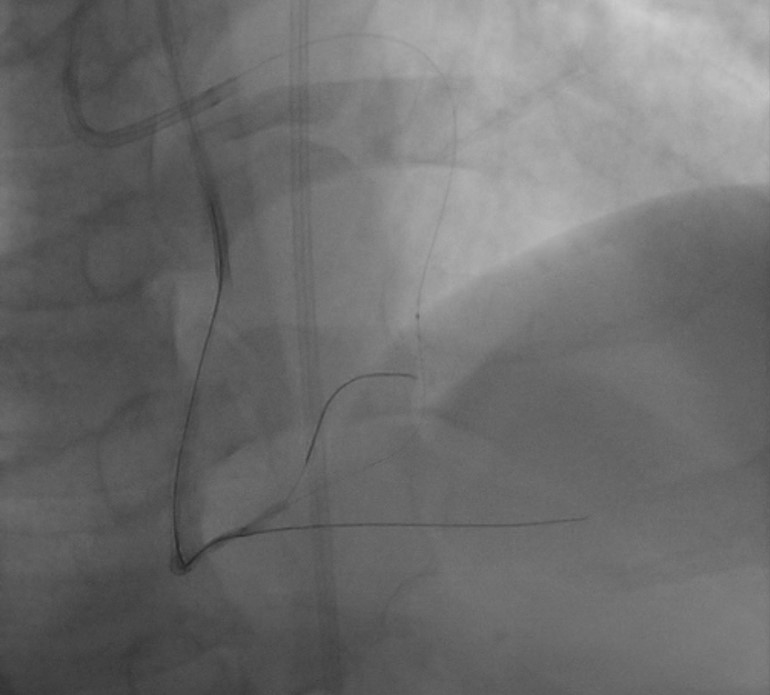
We perform PCI for distal RCA CTO part this time with bi-directional approaches. We use AL-1 6Fr with side-hole guiding catheter to engage RCA, and EBU 3.75 7Fr with side-hole to engage LCA. We tried antegrade approach initially with XT-A and APT microcatheter. The wire advanced to PDA lumen under the angiogram, and we use 2.0 mm balloon to dilate CTO part, and use cursade to advance another wire to PL branch. However, the wire didn't wire into PL lumen smoothly. We used IVUS to confirm the vessel condition. Though distal PDA wire was within the vessel, we discovered the wire went through a segmental false lumen at dRCA bifurcation, which extended to both PL and proximal PDA site. We began retrograde approach using Sion and Fielder FC wire with FineCross microcatheter via septal branch. The wire advance to PL smoothly, and successful externalization with RG3 was done. We then perform dRCA bifurcation kissing technique for PDA and PL branch, and deployed a drug-eluting stent at dRCA. Final angiogram showing good RCA distal flow without septal branch injury.

Case Summary
Both angiography and IVUS showing successful RCA CTO revascularization and salavage of bifurcation false lumen. We then performed dRCA bifurcation kissing technique for PDA and PL branch, and deployed a drug-eluting stent at dRCA. Final angiogram showing good RCA distal flow without septal branch injury.