
Lots of interesting abstracts and cases were submitted for TCTAP 2022. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-121
PTCA to Native LAD Through LIMA Graft Using Drug Eluting Balloon and Native LCX in a Post CABG Patient With Patent Grafts
By Saurabh Goel
Presenter
Saurabh Goel
Authors
Saurabh Goel1
Affiliation
Wockhardt Hopsital, Mumbai Central, India1,
View Study Report
TCTAP C-121
CORONARY - Drug-Eluting Balloons
PTCA to Native LAD Through LIMA Graft Using Drug Eluting Balloon and Native LCX in a Post CABG Patient With Patent Grafts
Saurabh Goel1
Wockhardt Hopsital, Mumbai Central, India1,
Clinical Information
Patient initials or Identifier Number
AH
Relevant Clinical History and Physical Exam
61 year old male, diabetic had anteroseptal MI in 2014 . He underwent CABG with LIMA RIMA Y graft to LAD and Ramus and SVG graft to right coronary artery. Since 2 months he complained of progressive exertional breathlessness.
Relevant Test Results Prior to Catheterization
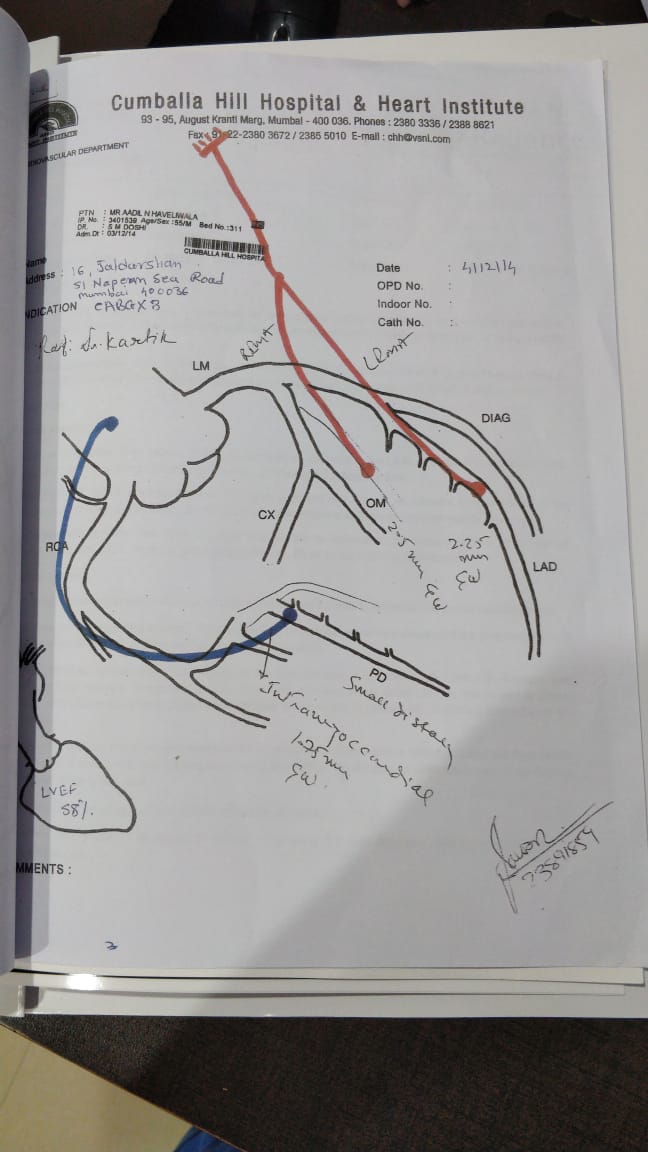
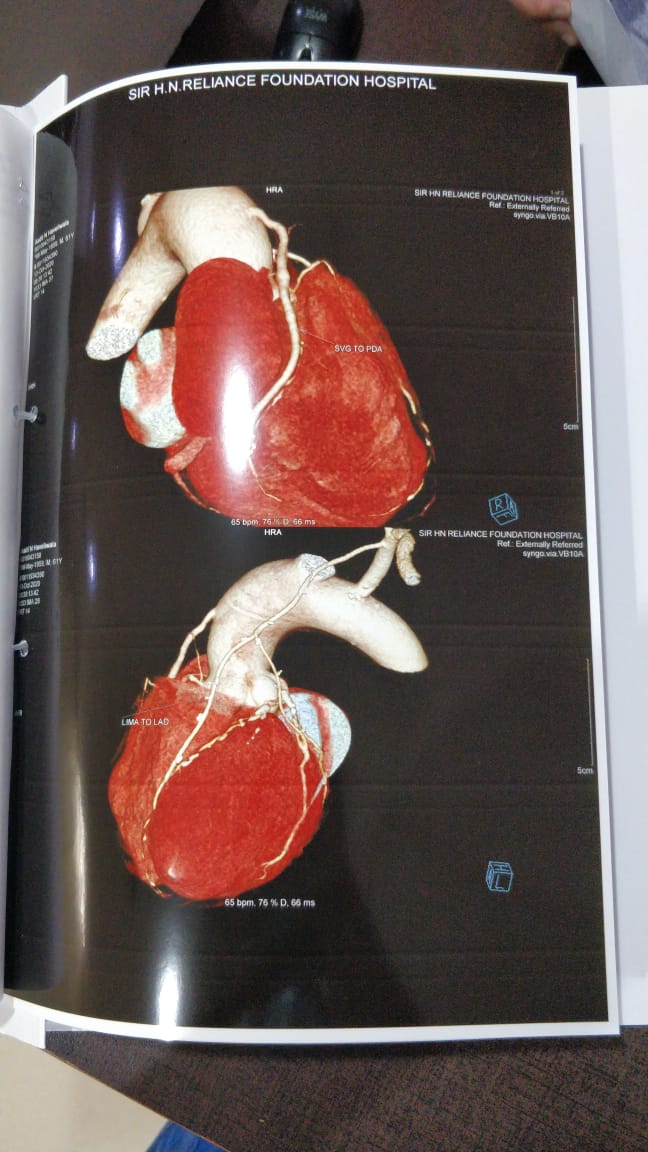
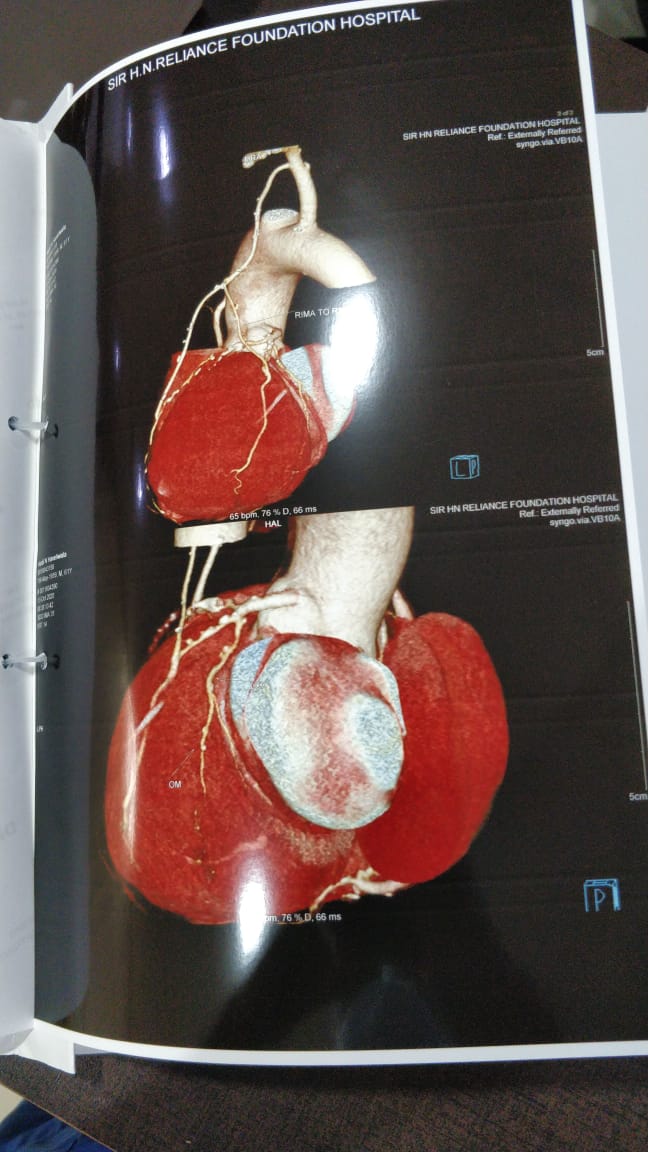
2 d echo showed LV ejection fraction of 50% with apicolateral hypokinesia.Treadmill stress test was positive for ischemia.CT Coronary angiography showed all grafts patent with disease in native LAD distal to LIMA graft anastomosis and disease in native ungrafted portion of LCX.
Relevant Catheterization Findings
Coronary angiography showed proximal LAD total occlusion and high grade lesion at ostium of Ramus. Native LCX showed significant proximal and mid disease. LIMA – RIMA graft to LAD and ramus was patent. Distal LAD showed severe disease beyond anastomosis. SVG graft to distal RCA was patent.
 3 CAG LEFT CORONARY.avi
3 CAG LEFT CORONARY.avi
5 GRAFT SVG to PDA.avi
7 Y GRAFT LIMA to LAD,OM.avi
Interventional Management
Procedural Step
PTCA to native distal LAD and native LCX was done. As proximal LAD was totally occluded PTCA done through LIMA using special LIMA guiding catheter. Sion blue wire was passed distally and balloon dilatation done using 2 X 20mm maverick balloon. This was followed by balloon dilatation using 2.25 X 40 mm Magic touch drug eluting balloon. A small area of dissection was noted at the lesion site and hence 2.25X 28 mm Xience Xpedition stent was deployed with good final result. Thereafter PTCA to native LCX was done using 2.5 X 33 and 2.5 X 18 mm Xience Xpedition stents with good final result. The patient experienced significant symptom relief after the procedure.
12 PTCA to LIMA-LAD MAGIC TOUCH 2.25 x 40 MM.avi
15 PTCA to LIMA-LAD AFTER STENTING 1.avi
20 final result.avi
Case Summary
Significant coronary lesions after CABG in ungrafted parts of distal and smaller vessels can often cause significant symptoms due to ischemia. This case illustrates how ungrafted smaller vessels were treated with drug eluting balloon and stents. A long Drug eluting balloon allows treatment of small distal vessels and here a smaller stent was later placed in an small area of dissection with good result. The distal LAD was treated through the LIMA graft using special LIMA guide catheter.