
Lots of interesting abstracts and cases were submitted for TCTAP 2022. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-146
Successful Revascularization Using Extreme Antegrade Guidewire Crossing by Anteowl Wr Intravascular Ultrasound Guided Parallel Wiring for Poor Run-off Cases of Continuous Occlusion From Superficial Femoral Artery to Bellow The Knee Artery
By Naoki Hayakawa
Presenter
Naoki Hayakawa
Authors
Naoki Hayakawa1
Affiliation
Asahi General Hospital, Japan1,
View Study Report
TCTAP C-146
ENDOVASCULAR - Peripheral Vascular Disease and Intervention
Successful Revascularization Using Extreme Antegrade Guidewire Crossing by Anteowl Wr Intravascular Ultrasound Guided Parallel Wiring for Poor Run-off Cases of Continuous Occlusion From Superficial Femoral Artery to Bellow The Knee Artery
Naoki Hayakawa1
Asahi General Hospital, Japan1,
Clinical Information
Patient initials or Identifier Number
JT
Relevant Clinical History and Physical Exam
A 76-year-old female with diabetesmellitus presented with rest pain and cyanosis of the both lower limbs. BMI was35.6. Her ambulatory status was mainly wheelchair due to contracture of the knee joint and obesity. Her ankle-brachial index (ABI)couldn’t be measured in both legs.
Relevant Test Results Prior to Catheterization
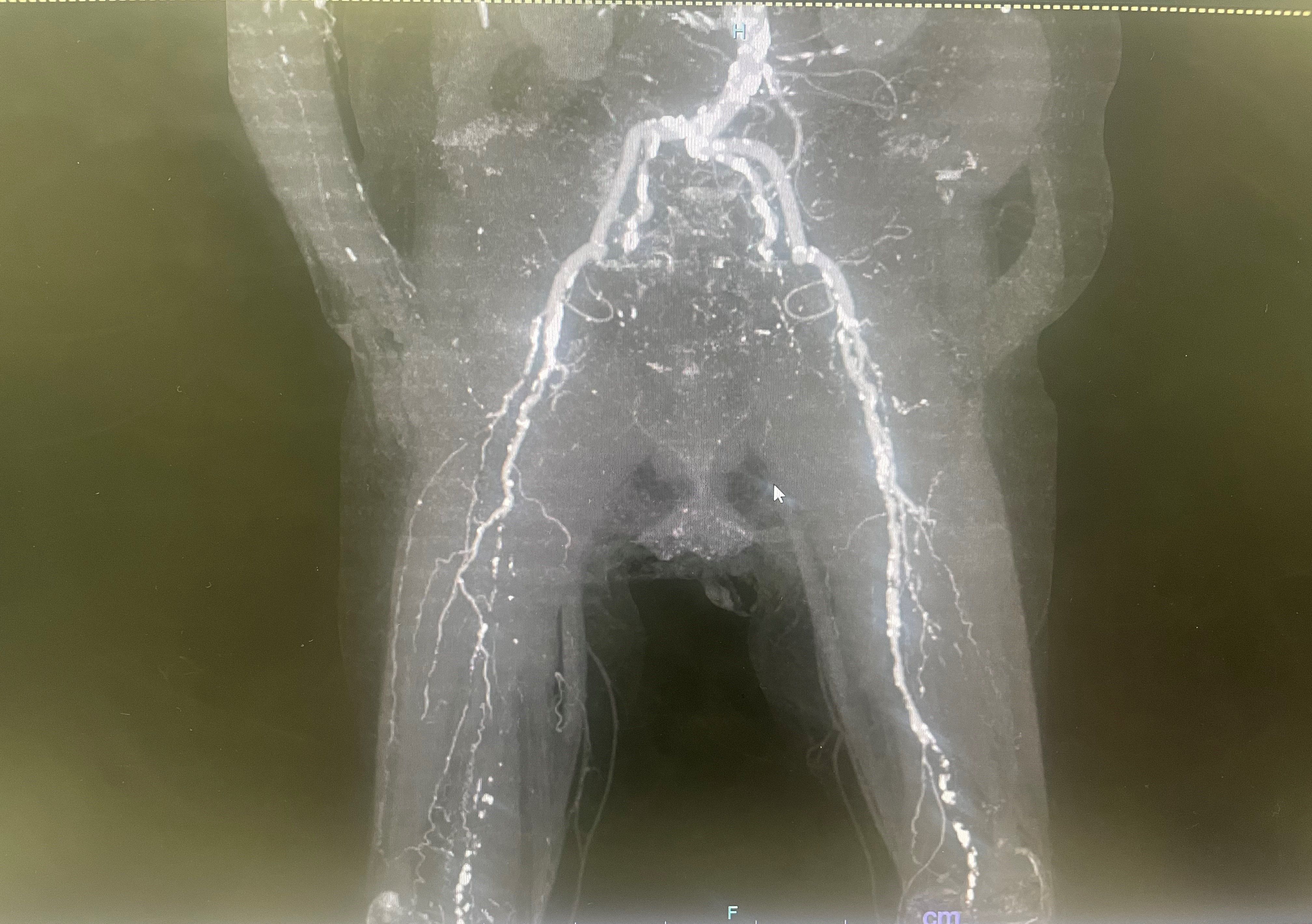
Contrast-enhanced computedtomography (CT) showed total occlusion of right superficial femoral artery(SFA) to popliteal artery (PopA) to bellow the knee (BTK) arteries. And severe stenosis of left SFA proximal, CTO from left SFA distal to BTK arteries. There were several calcification in both femoropopliteal arteries. Moreover, the bifurcation of SFA and deep femoral artery (DFA) was very high take-off, and iliac arteries were very torchuous.
Relevant Catheterization Findings
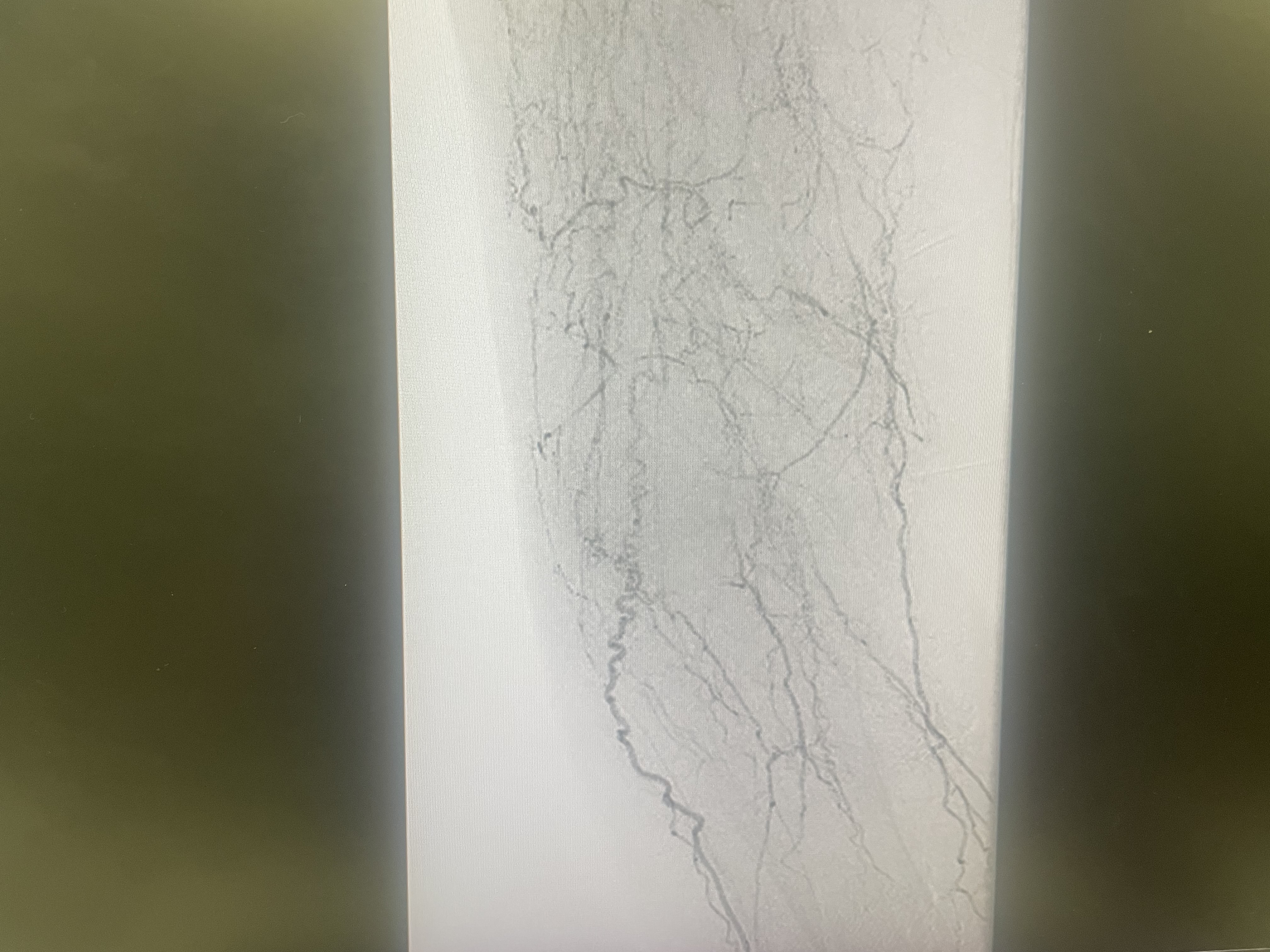
We inserted 6Fr Crossroads guiding-sheath from left common femoralartery. Angiography showed moderate stenosis of EIA distal, from SFA just proximal to BTK arteries. The distal dorsal pedis artery (DPA) was barely imaged, but the main trunk of tibial and peroneal was not imaged at all, and many collaterals were observed. Before wiring to the FP CTO, we dilated EIA stenosis with a 7.0mm balloon and guiding-sheath was advanced.
Interventional Management
Procedural Step
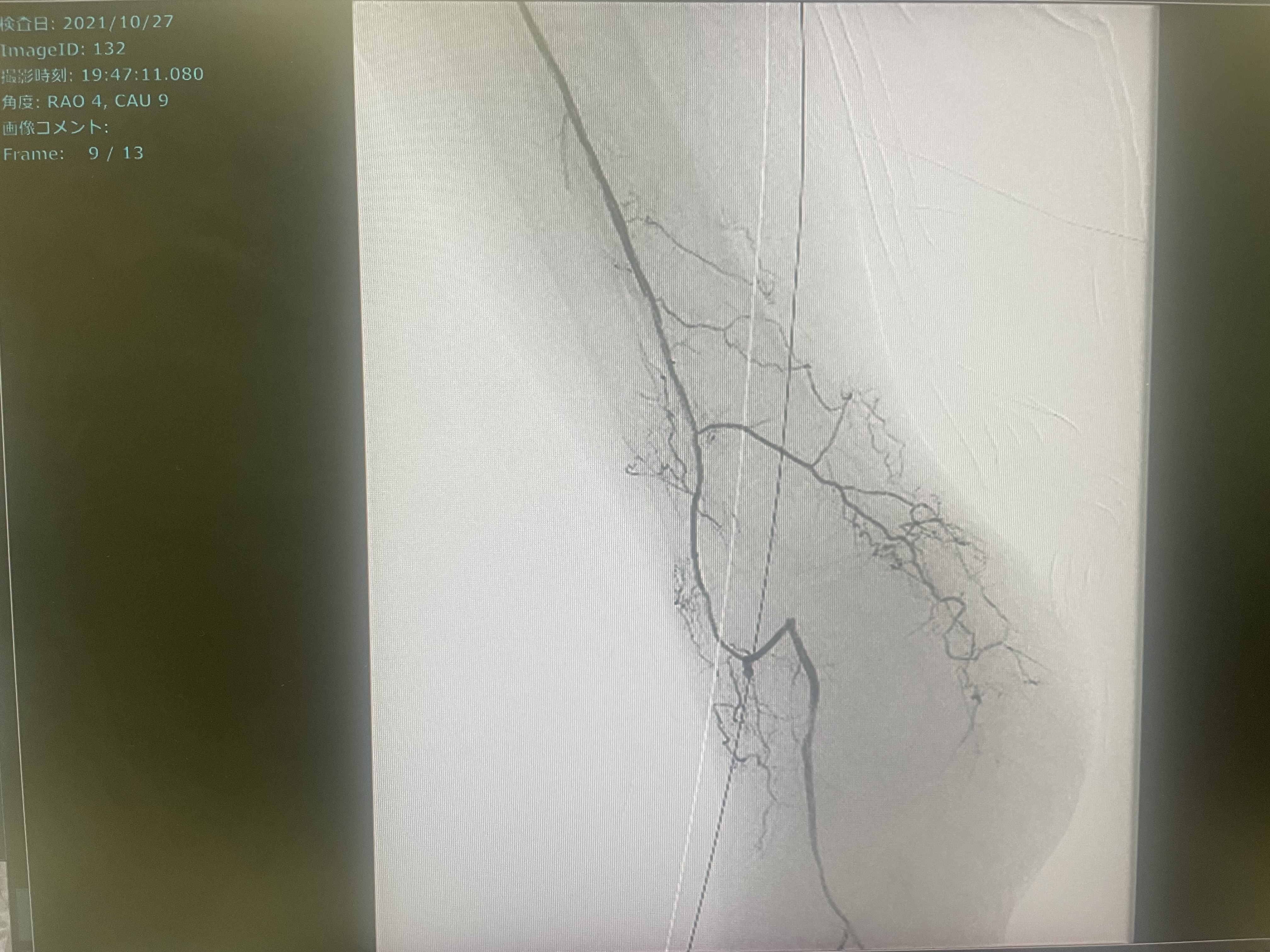
We advanced 10g 0.014-inch guidewire with 2.6Fr micro-catheter to SFA CTO. However, the guidewire couldn't be advanced from proximal Pop A.When AnteOwl WR(AnteOwl) IVUS was inserted atthe proximal PopA, it was subintimal from SFA mid, so IVUS guided parallel wiring was started using 40g 0.014-inch guidewire. AnteOwl is a novel IVUS for CTOintervention because of its unique structure. We can easily convert IVUS images into angiographic images for navigating the second guidewire through an intraplaqueroute under IVUS observation. We advanced the guidewire into the intraplaque route and could reach the distal popliteal artery. However, the total occlusion was continued to BTKarteries.Then, we advanced 3g 0.014-inch guidewire with small knuckle shape to peroneal artery. IVUS could be advanced distally and was subintimal from the peroneal entrance. By repeating these steps of IVUS guided parallel wiring several times, we finally succeeded in passing it through the distal true lumen. Tip injection confirmed that the distal true lumen of the peroneal was connected to the DPA via a collateral tract.1 Epic bare nitinol stent was deployed for EIA, 4 Eluvia drug-eluting stent for PopA toSFA, 1 Ranger drug-coated balloon for PopA, and balloon dilation for peroneal artery. Final angiography showed very good antegrade flow.PostoperativeABI improved to 0.9, and a good clinical course has been obtained.

Case Summary
Sometimesretrograde approach such as distal puncture is difficult in patient with poor-distal run-off. Even after subintimal long stenting including BTK, there are problems such as patency and loss of side small branches. This time, we experienced a case in which the new IVUS was used to pass through all true lumen antegradely, and revascularization was successful. We have named this technique the excavator technique (EXtreme antegrade guidewire Crossing to distal true lumen with AnteOwl WR intraVAscular ulTrasOund guided paRallel wiring to a bellow the knee artery) and have recently been challenging the poor-run off case, so we will report it.