
Lots of interesting abstracts and cases were submitted for TCTAP 2022. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-151
Left Main Coronary Artery Stent Deformity Caused by Dilated Sinus of Valsalva Compression
By Jiunn-Wen Lin, William Kongto Hau
Presenter
Jiunn-Wen Lin
Authors
Jiunn-Wen Lin1, William Kongto Hau2
Affiliation
Tzu-Chiz General Hospital, Taiwan1, The Chinese University of Hong Kong, Hong Kong, China2,
View Study Report
TCTAP C-151
IMAGING AND PHYSIOLOGIC LESION ASSESSMENT - Imaging: Intravascular
Left Main Coronary Artery Stent Deformity Caused by Dilated Sinus of Valsalva Compression
Jiunn-Wen Lin1, William Kongto Hau2
Tzu-Chiz General Hospital, Taiwan1, The Chinese University of Hong Kong, Hong Kong, China2,
Clinical Information
Patient initials or Identifier Number
S.S. Chen
Relevant Clinical History and Physical Exam
A 78-year-old male with a history of hypertension under medical therapy presented with effort angina. Physical examination revealed diastolic blowing murmur on the left lower sternal border. CxR revealed cardiomegaly with dilated ascending aorta.

Relevant Test Results Prior to Catheterization
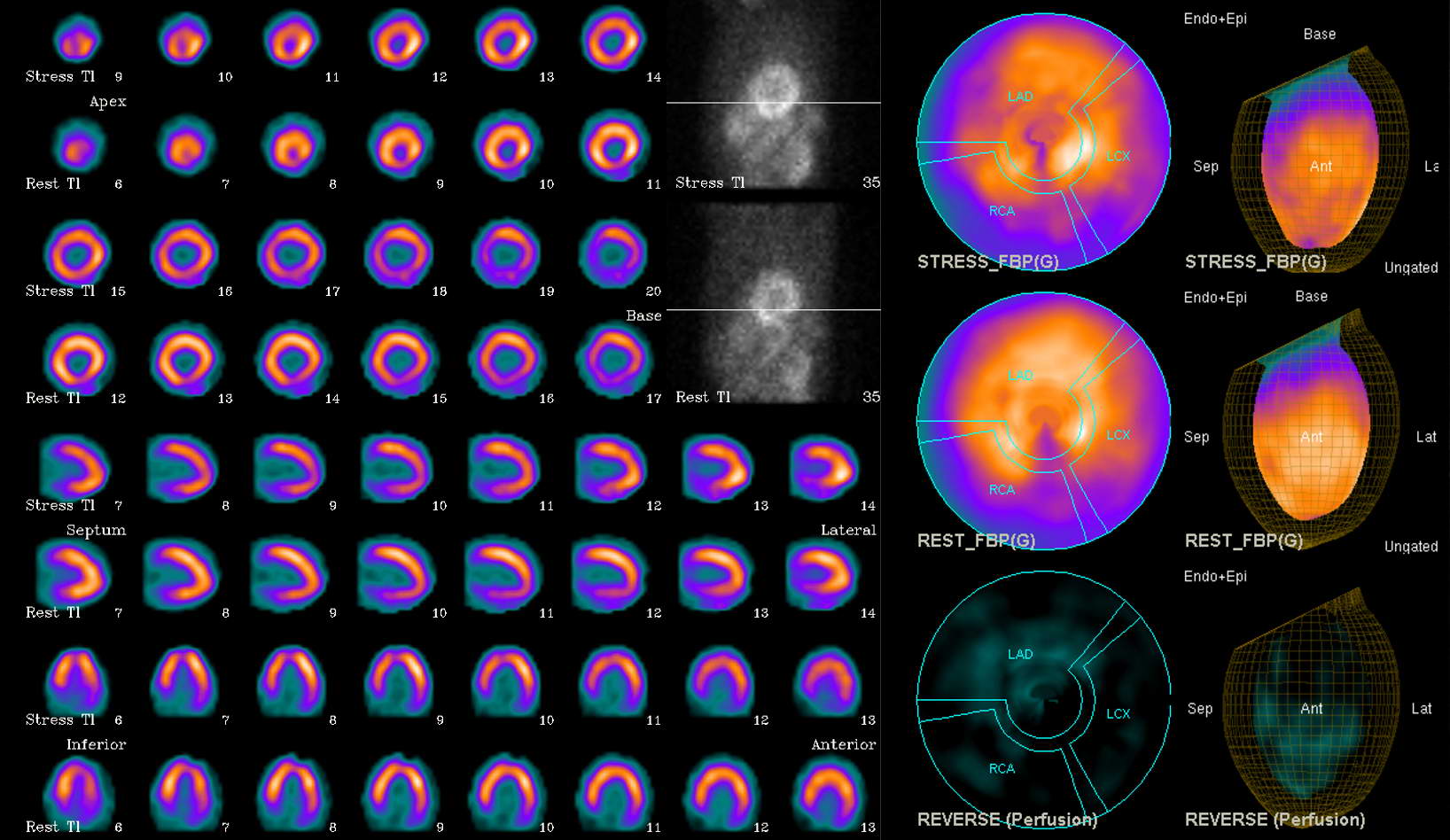
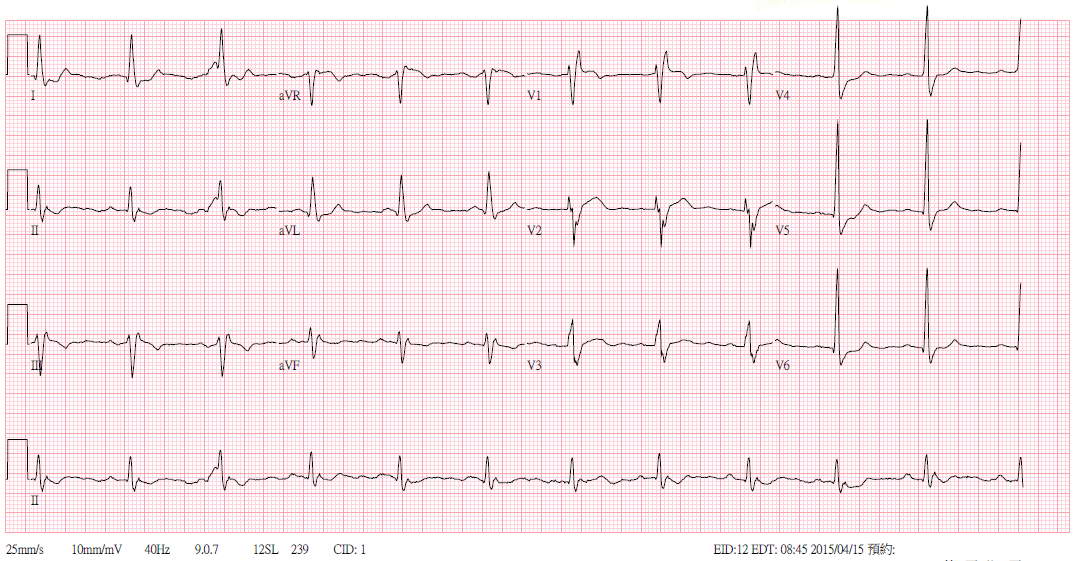
ECG revealed RBBB and non-specific ST-T change. Thallium scan revealed perfusion defects in apical, anteroseptal and inferior walls.
Relevant Catheterization Findings
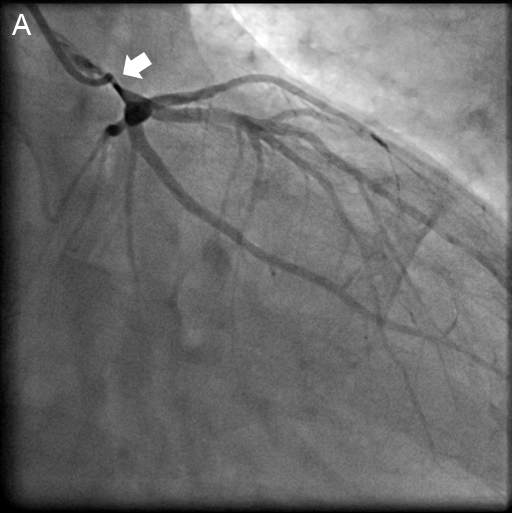
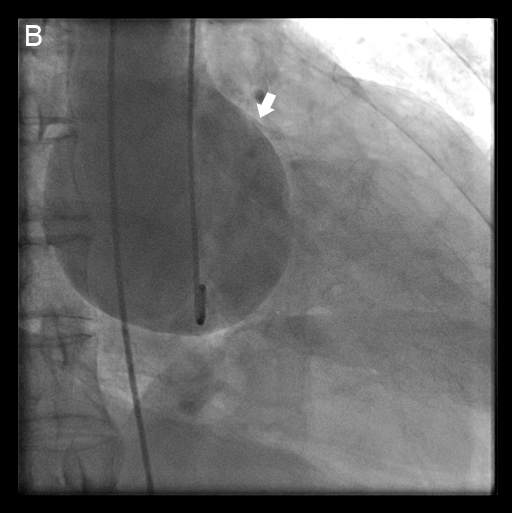
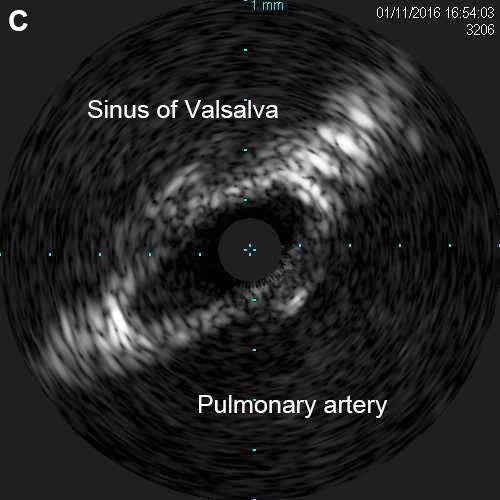
Coronary angiography revealed severe stenosis in the left main coronary artery (LMCA) without significant atherosclerosis in other coronary segments (Fig. 1A). Aortogram revealed a dilated aortic root, pushing the LMCA up towards the pulmonary artery (Fig. 1B). Intravascular ultrasound (IVUS) revealed an asymmetric oval-shaped lumen due to compression of the pulmonary artery and sinus of Valsalva (Fig. 1C).
Interventional Management
Procedural Step
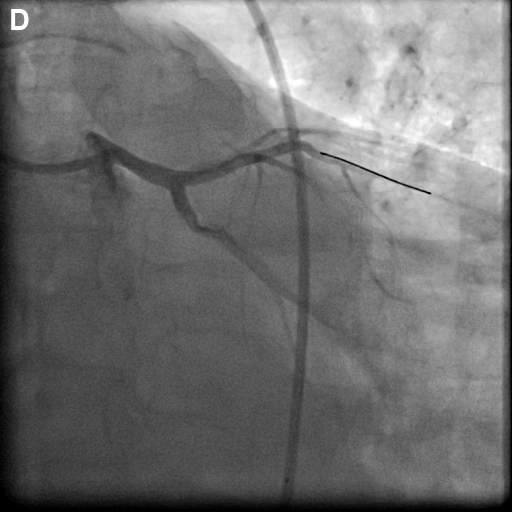
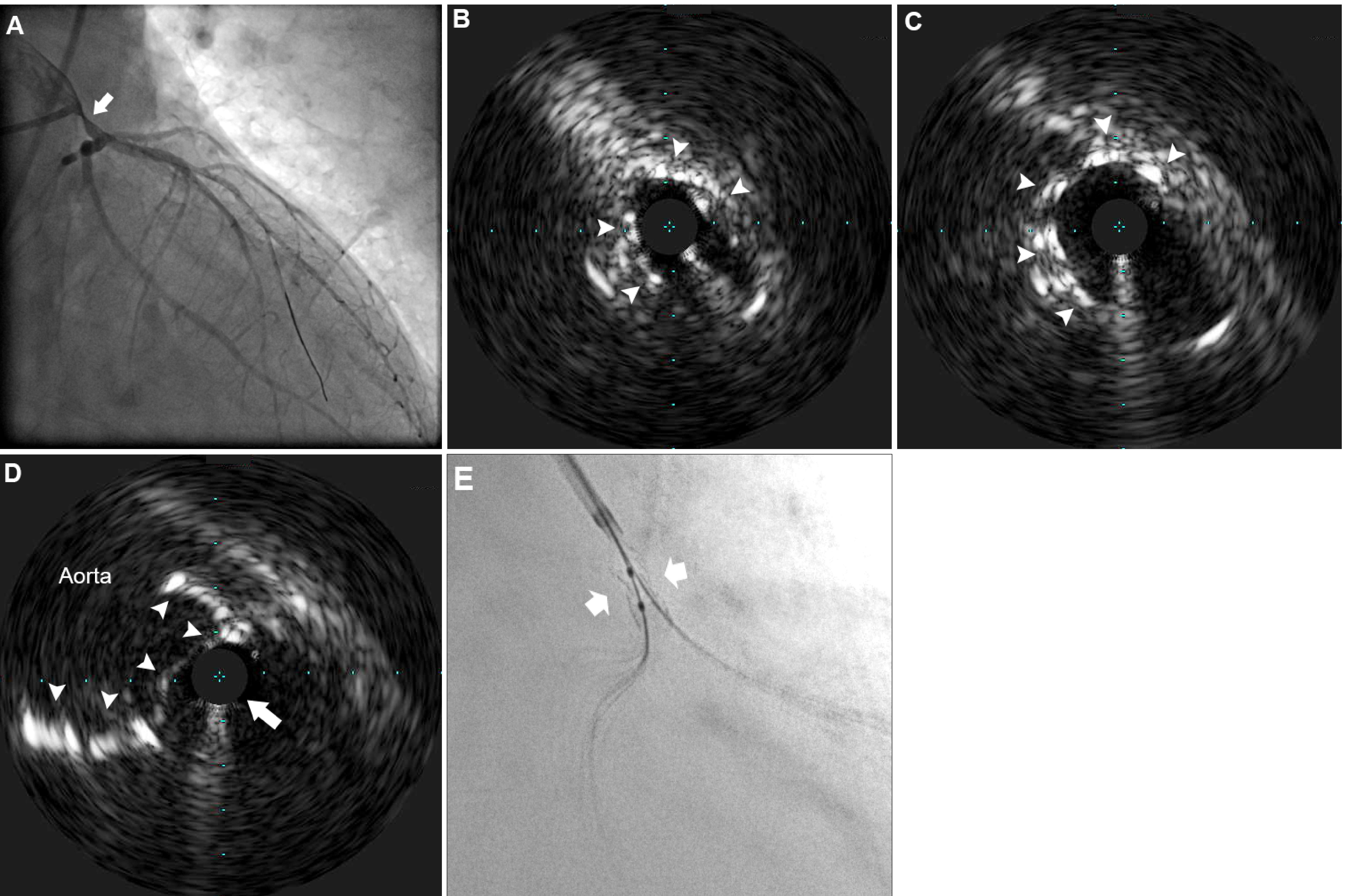
A drug-eluting stent (4.0x12 mm) was deployed at the site of LMCA stenosis (Fig. 1D). The patient’s symptoms were relieved and was discharged with standard medications. Three months later, the patient suffered from Non-ST elevation myocardial infarction. Coronary angiography revealed restenosis in the previous LMCA stent (Fig. 2A). IVUS revealed an oval-shaped stent configuration between the sinus of Valsalva and pulmonary artery (Fig. 2B). IVUS demonstrated stent struts were missing over an arc of approximately 150°, indicating stent fracture (Fig. 2B-C). A protruding stent from the LMCA ostium with IVUS probe outside the stent was also observed (Fig. 2D). Discontinuity of the stent strut was observed indicative of stent fracture (Fig. 2E), caused by the extrinsic compression of the dilated sinus of Valsalva. Bentall procedure was performed with concomitant coronary artery bypass grafting and an uneventful post-operation course.
Case Summary
Extrinsic compression of the LMCA is an increasingly recognized disease entity, primarily in patients with pulmonary hypertension with a dilated pulmonary artery. Percutaneous coronary intervention with stenting should be avoided considering the high compression force generated by the dilated sinus of Valsalva, which predisposes the stent to deformation.