
Lots of interesting abstracts and cases were submitted for TCTAP 2022. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-080
Looks Can Be Deceiving : A Case of Retrograde Approach With Reverse Cart in Elderly Patient
By Doreen Sumpat, Azrina Abdul Kadir, Hou Tee Lu
Presenter
Doreen Sumpat
Authors
Doreen Sumpat1, Azrina Abdul Kadir2, Hou Tee Lu2
Affiliation
Universiti Malaysia Sabah, Malaysia1, Sultanah Aminah Hospital, Malaysia2,
View Study Report
TCTAP C-080
CORONARY - Complex and Higher Risk Procedures for Indicated Patients (CHIP)
Looks Can Be Deceiving : A Case of Retrograde Approach With Reverse Cart in Elderly Patient
Doreen Sumpat1, Azrina Abdul Kadir2, Hou Tee Lu2
Universiti Malaysia Sabah, Malaysia1, Sultanah Aminah Hospital, Malaysia2,
Clinical Information
Patient initials or Identifier Number
SH
Relevant Clinical History and Physical Exam
SH, a 64-year old man with Type 2 diabetes mellitus and hypertension. He was also a chronic smoker. He was symptomatic with exertional dyspnea and exertional angina CCS II for past six months. These symptoms became worsened for past one month prior to admission and was partially relieved despite on optimized antianginal medication. However, he had no failure symptoms and clinical examination was unremarkable.

Relevant Test Results Prior to Catheterization
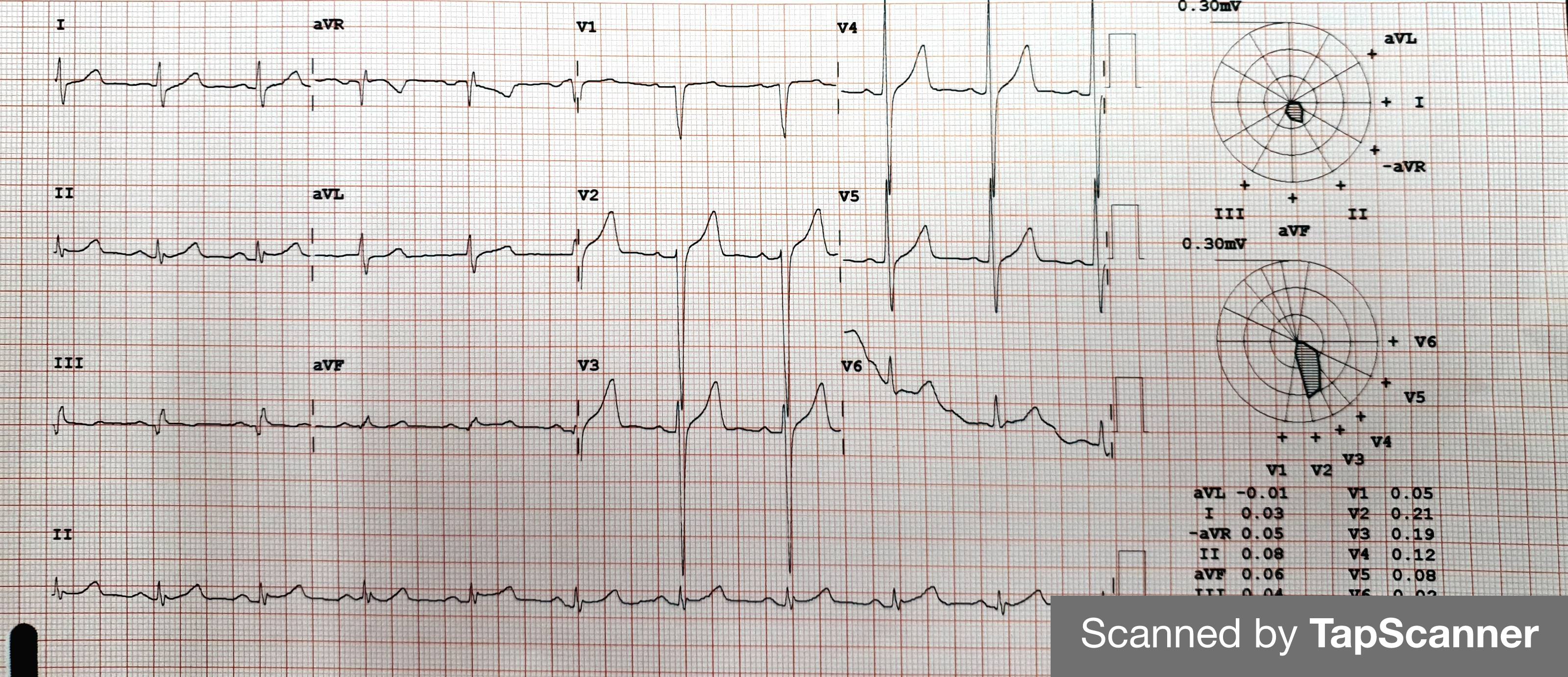
His bloodresult were all normal. He had no anemia and renal function was within normallimit. Electrocardiogram showed no ischemic changes or rhythm abnormalities. Despite his symptoms, echocardiogram revealed preserved left ventricular function with no regionalwall abnormalities. Chambers size and wall thickness were normal. There was no valvular abnormalities as well.
Relevant Catheterization Findings
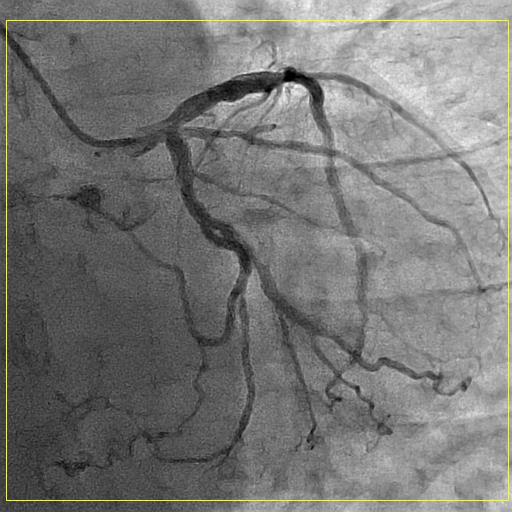
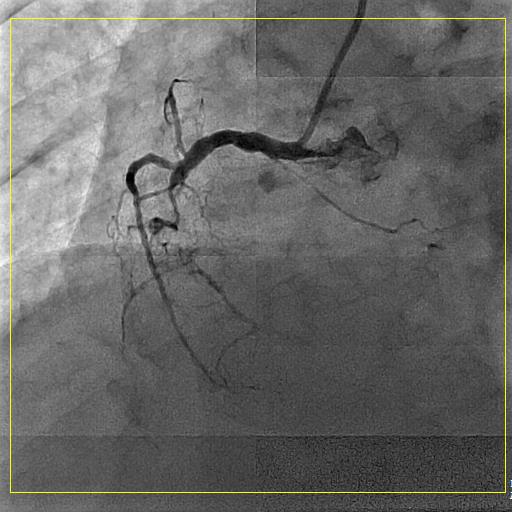
Coronary angiogram was performed via right radial artery with Optitorque. Coronary angiogram showed single vessel disease with mid-RCA had chronic total occlusion with collaterals from septal branches. Proximal LAD showed 30-40% stenosis and proximal LCX showed 20-30% stenosis. Therefore, after discussion with patient and consent was granted, a staged PCI to mid-RCA was performed in view of his symptoms.
 SCH Video1.avi
SCH Video1.avi
SCH Video2.avi
SCH Video3.avi
Interventional Management
Procedural Step
Procedure done via both femoral access. 7Fr AL1 guidingcatheter was engaged to right coronary ostium and 6Fr EBU 3.5 guiding catheterto left coronary ostium. Antegrade approach initially attempted with FielderXT-R and Mogul microcatheter but failed to cross proximal cap mRCA CTO.Retrograde approach attempted with first septal branch was wired with Sion Blueand Caravel microcatheter but failed too. Decided to shift strategy to reverseCART. Predilatation from pRCA up to proximal cap mRCA CTO was done withSapphire II Pro 1.5 x 10mm and Euphora 2.0 x 10mm balloon. This was tofacilitate knuckled wire technique with Fielder XT-R to reach subintimal planeof occlusion. Aggressive antegrade dilatation of CTO lesion at subintimal planewith same balloon at nominal pressure for successful navigation of retrogradewire. The balloon also placed partially back into the true lumen and inflated.Ultimate Bros 3 as retrograde wire with Caravel microcatheter supportsuccessfully crossed distal cap, entered subintimal plane into proximal truelumen. True lumen confirmed with tip injection via microcatheter and biplaneview. Externalization retrogradely with RG3 with Caravel microcatheter.Antegrade wire exchange to RUNTHROUGH floppy. Predilatation with Scoreflex NC2.5 x 20mm from mRCA to PDA. Stented dRCA to PDA with Resolute Integrity 2.25 x30mm. Stented mRCA with Biomatrix Alpha 2.75 x 36mm and overlapped it withdistal stent. End result was good, no dissection and TIMI 3 flow.
SCH Video5.avi
SCH Video7.avi
video.avi
Case Summary
Retrograde approach and reverse CART in complex PCI is possible with basic tools without IVUS guided. Mastering of knuckled wire technique for subintimal plane entry is upmost important in this case. Aggressive antegrade balloon dilatation with care is vital to facilitate entry of retrograde wire. Ideally, tip of retrograde microcatheter lies in midportion of antegrade balloon. Antegrade balloon and retrograde catheter may appear 4–5 mm apart on fluoroscopy. Avoid antegrade contrast injections after creation of antegrade subintimal dissection until last stent is deployed. This is to prevent spiral dissection or hematoma and extending it downstream. It is safe and reproducible technique.