
Lots of interesting abstracts and cases were submitted for TCTAP 2022. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-057
How to Overcome Acute Bend in Antegrade Proximal Circumflex In-Stent Chronic Total Occlusion
By Entzu Liu, Hsien-Li Kao
Presenter
Entzu Liu
Authors
Entzu Liu1, Hsien-Li Kao1
Affiliation
National Taiwan University Hospital, Taiwan1,
View Study Report
TCTAP C-057
CORONARY - Chronic Total Occlusion
How to Overcome Acute Bend in Antegrade Proximal Circumflex In-Stent Chronic Total Occlusion
Entzu Liu1, Hsien-Li Kao1
National Taiwan University Hospital, Taiwan1,
Clinical Information
Patient initials or Identifier Number
Qin
Relevant Clinical History and Physical Exam
A 73-year-old man presented with recurrent angina. PCI with DES at both LCX and RCA was done 6 years ago. His coronary risk factors included hypertension, type 2 diabetes mellitus and dyslipidemia. Physical examination was unremarkable.
Relevant Test Results Prior to Catheterization
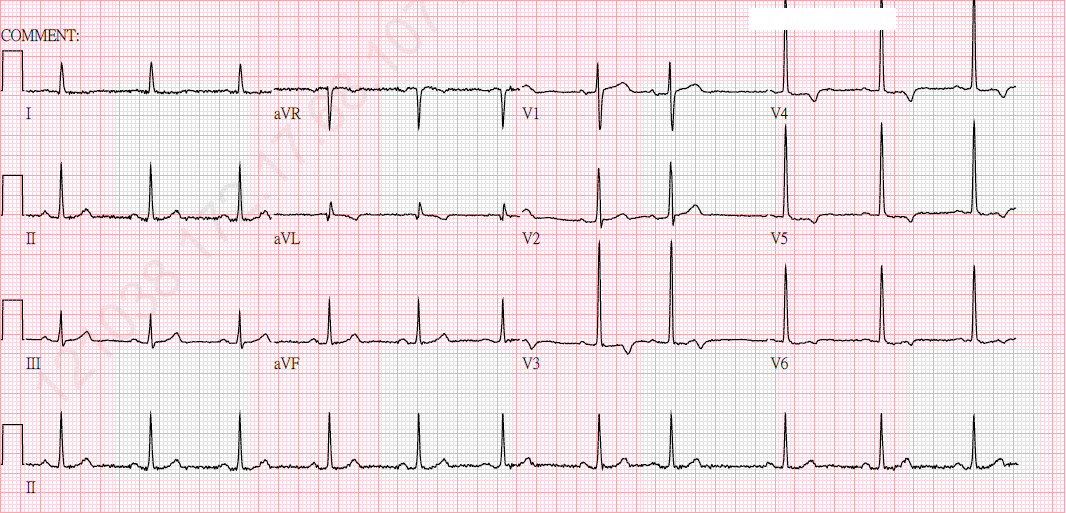
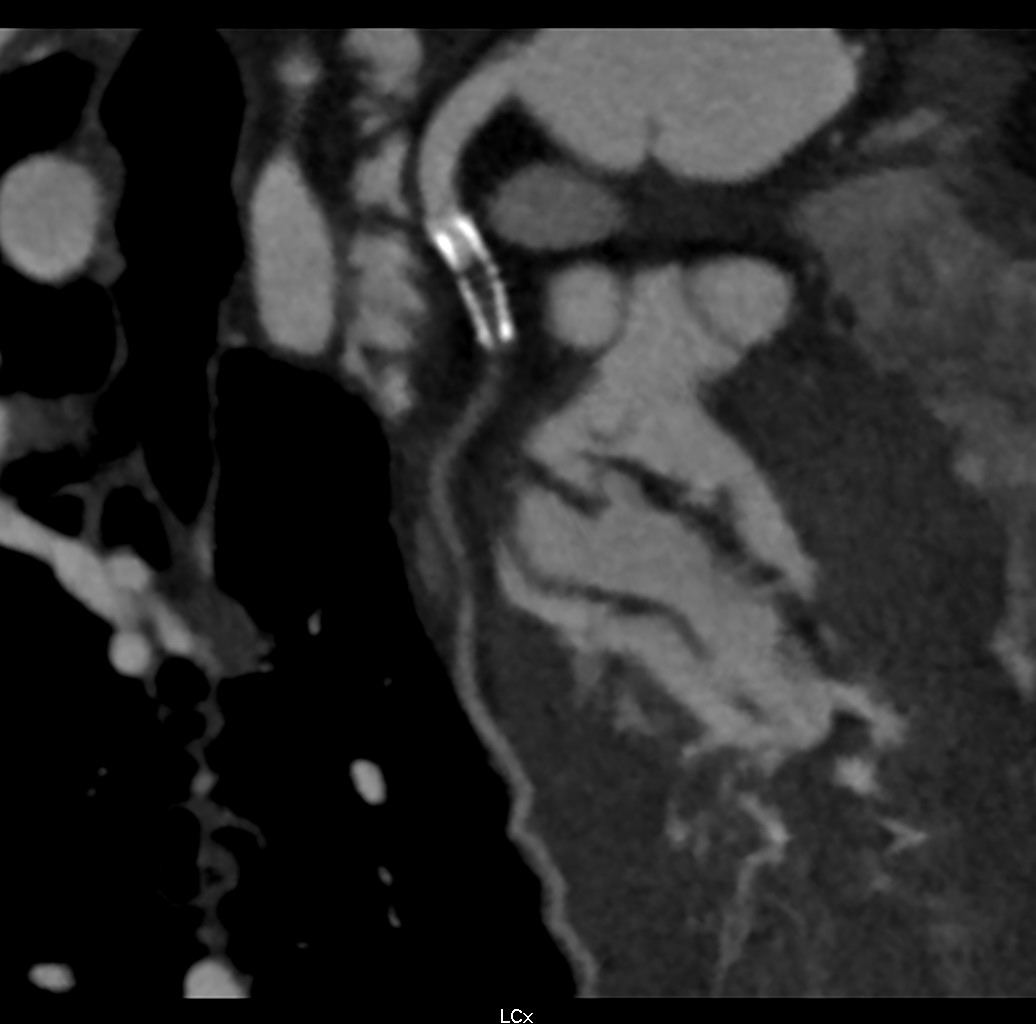
Electrocardiogram showed normal sinus rhythm with T wave inversion in lead aVL, V3-V6. Echocardiography revealved preserved ejection fraction of 80% and no regional wall motion abnormality. Exercise stress testing showed positive results. CT angiography revealed in-stent total occlusion at proximal LCX, moderate (50%-69%) stenosis at middle LCX and mild (25%-49%) stenosis at middle LAD and proximal RCA.
Relevant Catheterization Findings
LM: PatentLAD: PatentLCX: proximal ISR CTO with extreme retroflex angulation from LM to LCXRCA: proximal ISR 30 %, middle stenosis 30 %, PDA No ISR, with collateral to LCX
 LCX RAO.mp4
LCX RAO.mp4
LCX Spidervies.mp4
RCA collateral to LCX.mp4
Interventional Management
Procedural Step
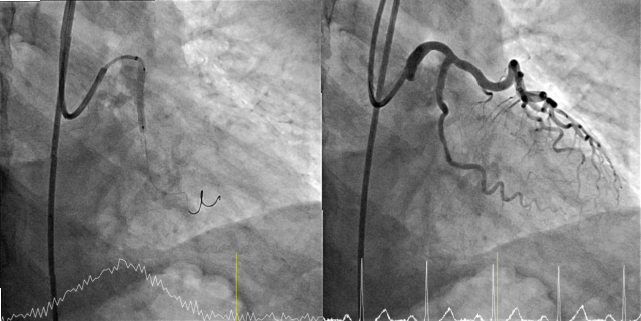
1. Used right femoral artery approach and engaged 7Fr BL 3.5 to LCA.2. Antegrade wiring with Sion Black and Ultimate bros 3 with Finecross support, but failed due to poor backup support.3. Further wiring with Ultimate bros 3/ Gaia second/ Gaia third with double lumen catheter Crusade support (with Sion Black in LAD) still failed.4. Gaia third advanced into LCX stent subintima, and then Corsair Pro pushed over Gaia second into proximal LCX, with2.5mm Ryurei balloon blocking proximal LAD.5. Gaia third was then exchanged to Gaia second and crossed the ISR CTO successfully.6. Tip injection from Corsair Pro confirmed distal true lumen, and wire changed to Sion Blue.7. Pre-dilatation POBA with Ryurei 1.5 x 15mm, but then Volcano Refinity IVUS delivery failed.8. 6 Fr Guiding extension catheter (Expressman) advanced into proximal LCX, followed by Ryurei 2.5mm and 3.5mm dilatation.9. IVUS catheter delivered to distal LCX, and then 2.25mm Agent DCB was applied after 2.25mm NSE Alpha in distal LCX. 10. 3.0mm Pantera Lux DCB was then applied after the same 2.25mm NSE Alpha in the proximal-distal LCX ISR.11. The final angiography showed a good result.
CTO pass.mp4
Tip injection confirmed distal true lumen.mp4
Case Summary
Acute bend in the vessel proximal to a CTO lesion increases the technical difficulty. Successful antegrade wiring with good microcatheter support and blocking balloon in a proximal side branch to prevent system prolapsing may help.