
Lots of interesting abstracts and cases were submitted for TCTAP 2022. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-098
Horrible Injection !!! " Aorto-Coronary Dissection "
By Ramy Mohamed Atlm, Salma Mohamed Elshokafy
Presenter
Salma Mohamed E-lshokafy
Authors
Ramy Mohamed Atlm1, Salma Mohamed Elshokafy1
Affiliation
Tanta University Hospital, Egypt1,
View Study Report
TCTAP C-098
CORONARY - Complications
Horrible Injection !!! " Aorto-Coronary Dissection "
Ramy Mohamed Atlm1, Salma Mohamed Elshokafy1
Tanta University Hospital, Egypt1,
Clinical Information
Patient initials or Identifier Number
A S
Relevant Clinical History and Physical Exam
´ Female patient aged 61 years old , Known diabetic ,Hypertensive , Dyslipidemic .
Relevant Test Results Prior to Catheterization
Ø ECG shows : Sinus Rhythm with T waveinversion and ST depression in infero-lateral leads
Relevant Catheterization Findings
According to Esc guidelines for Risk Stratification of NON-STEMI patients Our patient isconsidered high risk
* Dynamic ECG changes
* Elevated cardiac enzymes
So, Early invasive PCI in the first 24 hours was indicated
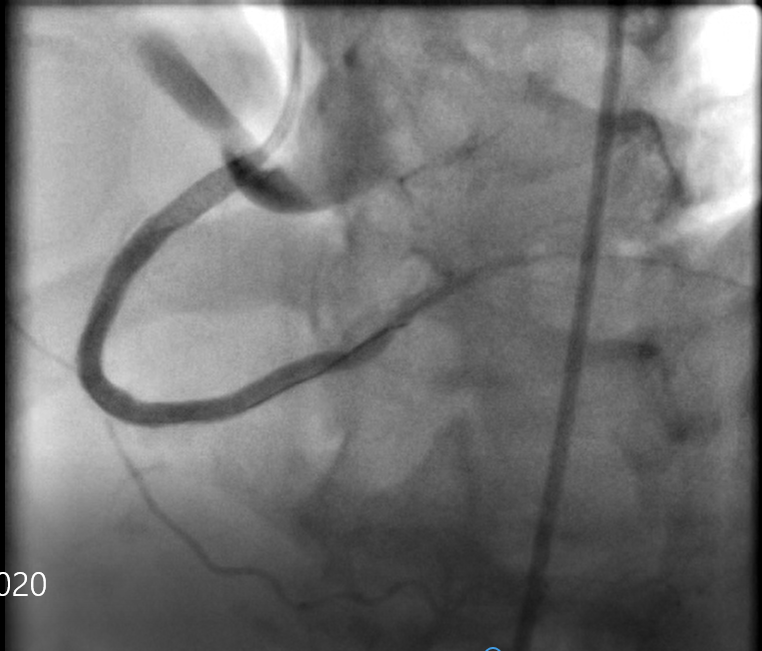
 Series_004_Coro 2020.wmv
Series_004_Coro 2020.wmv
* Dynamic ECG changes
* Elevated cardiac enzymes
So, Early invasive PCI in the first 24 hours was indicated
Interventional Management
Procedural Step
Engagement of RCA with JR 4 Guiding catheter
Wiring of RCA with PT2 MS guide wire over a 2 * 15 mm semi-complaint balloonsupport
of the dissection and to stop blood flow into false lumen
horrible injection , Aorto coronary dissection.pptx
Series_007_Coro 2020.wmv
Series_023_Coro 2020.wmv
Wiring of RCA with PT2 MS guide wire over a 2 * 15 mm semi-complaint balloonsupport
of the dissection and to stop blood flow into false lumen
Case Summary
´ Iatrogenic Catheter induced aorto-coronary dissection is rare but life threatening complication during PCI .