
Lots of interesting abstracts and cases were submitted for TCTAP 2022. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-058
Reattempt Antegrade CTO PCI Using Turnpike Spiral Catheter Followed by Drug Coated Balloons in De Novo Coronary Lesions Complicated With Iatrogenic Type B Coronary Artery Dissection
By Quah Wy Jin, Chan Ho Thum, Khai Chih Teh, Jayakhanthan Kolanthaivelu
Presenter
Quah Wy Jin
Authors
Quah Wy Jin1, Chan Ho Thum1, Khai Chih Teh1, Jayakhanthan Kolanthaivelu2
Affiliation
National Heart Institute, Malaysia1, Cardiovascular Sentral Kuala Lumpur, Malaysia2,
View Study Report
TCTAP C-058
CORONARY - Chronic Total Occlusion
Reattempt Antegrade CTO PCI Using Turnpike Spiral Catheter Followed by Drug Coated Balloons in De Novo Coronary Lesions Complicated With Iatrogenic Type B Coronary Artery Dissection
Quah Wy Jin1, Chan Ho Thum1, Khai Chih Teh1, Jayakhanthan Kolanthaivelu2
National Heart Institute, Malaysia1, Cardiovascular Sentral Kuala Lumpur, Malaysia2,
Clinical Information
Patient initials or Identifier Number
SAV
Relevant Clinical History and Physical Exam
A 59 years old gentleman with underlying diabetes mellitus, dyslipidaemia and history of cerebrovascular accident in 2017 (ADL dependent) presented with exertional dyspnoea for 2 months. He had no angina. Clinically, physical examination was unremarkable aside from minimal bilateral ankle edema.
Relevant Test Results Prior to Catheterization
LDL: 2.3 mmol/l, HDL: 2.0 mmol/Haemoglobin : 11.8 g/dlCreatinine: 80 umol/lHbA1c: 6.7 %
ECG showed sinus rhythm with right bundle branch block
Transthoracic Echocardiogram :Left ventricular ejection fraction (LVEF) : 60%No regional wall motion abnormalitiesNormal chamber sizes, no significant valve diseases
Myocardial perfusion scan showed large area of stress induced ischaemia in the RCA territory
 Diagnostic angiogram (LCx) part 1.mpg
Diagnostic angiogram (LCx) part 1.mpg
Diagnostic angiogram (LCx) part 2.mpg
Diagnostic angiogram (LCx) part 3.mpg
ECG showed sinus rhythm with right bundle branch block
Transthoracic Echocardiogram :Left ventricular ejection fraction (LVEF) : 60%No regional wall motion abnormalitiesNormal chamber sizes, no significant valve diseases
Myocardial perfusion scan showed large area of stress induced ischaemia in the RCA territory
Relevant Catheterization Findings
The index coronary angiogram showed normal left main with mild disease at proximal left anterior descending artery (LAD). The left circumflex artery (LCx) is dominant with chronic total occlusion at mid segment with retrograde collaterals from LAD and severe disease at the 2nd obtuse marginal branch. The right coronary artery (RCA) is small with severe disease proximally followed by chronic total occlusion.
Diagnostic angiogram (LAD) part 1.mpg
Diagnostic angiogram (LAD) part 2.mpg
Diagnostic angiogram (RCA).mpg
Interventional Management
Procedural Step
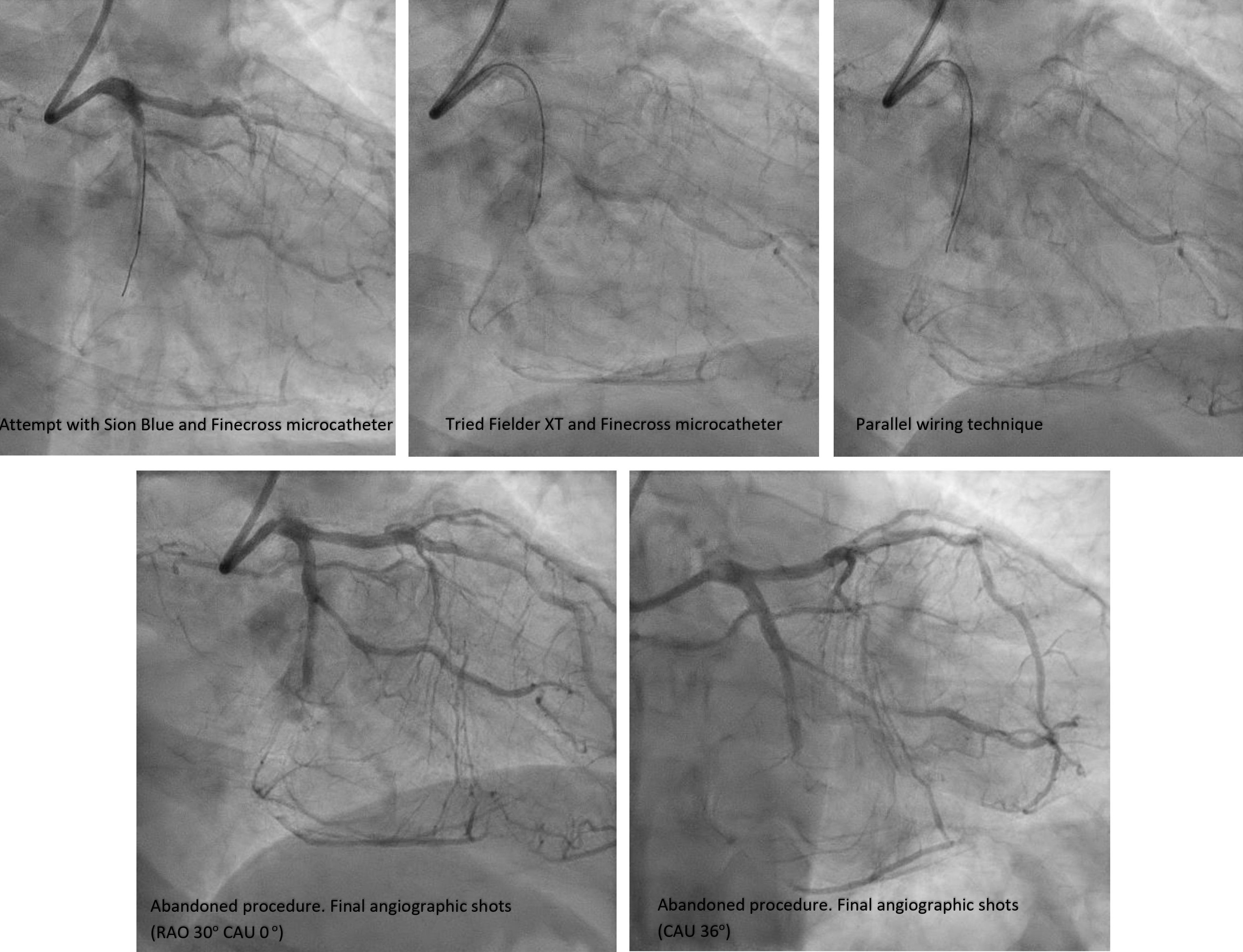
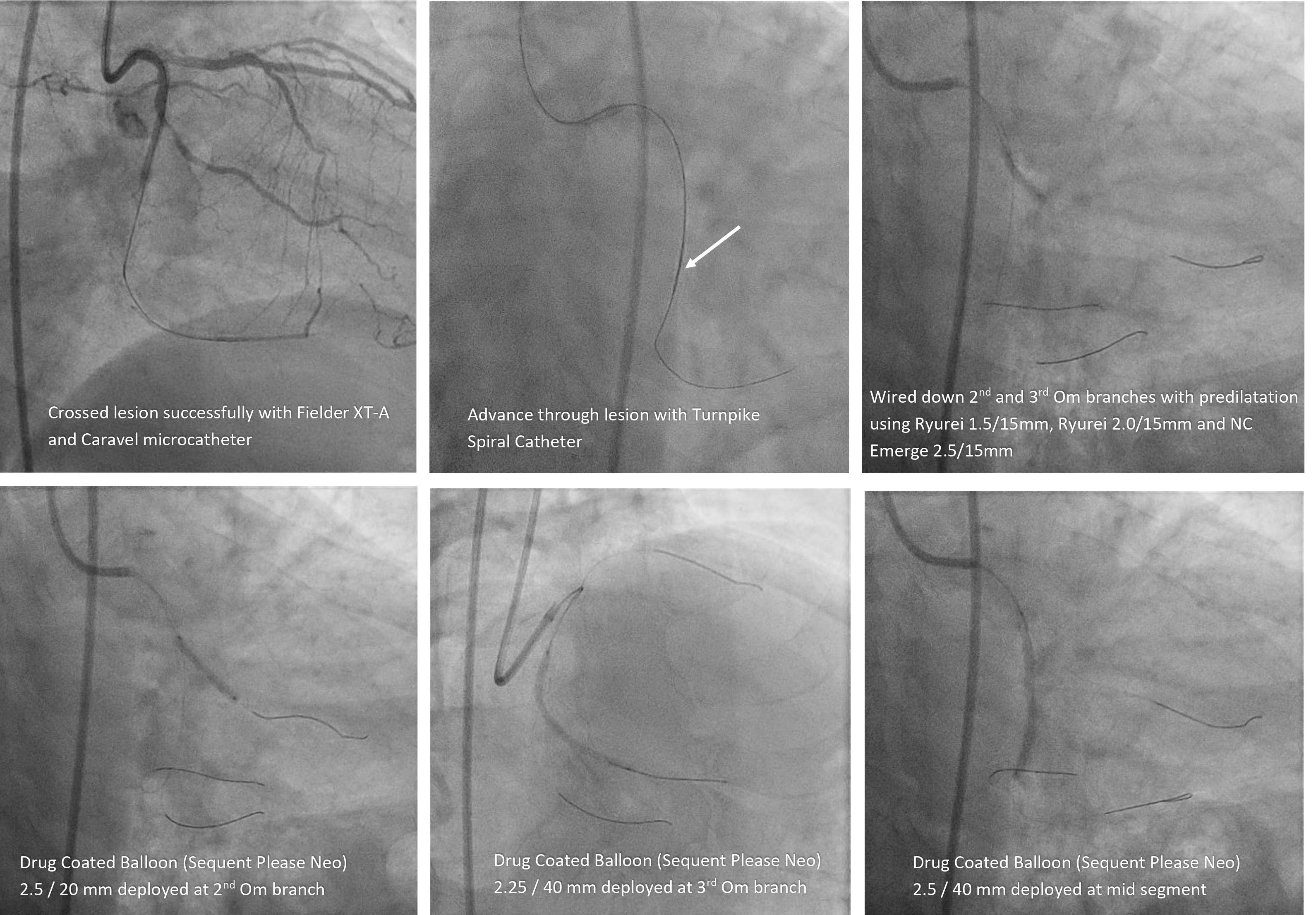
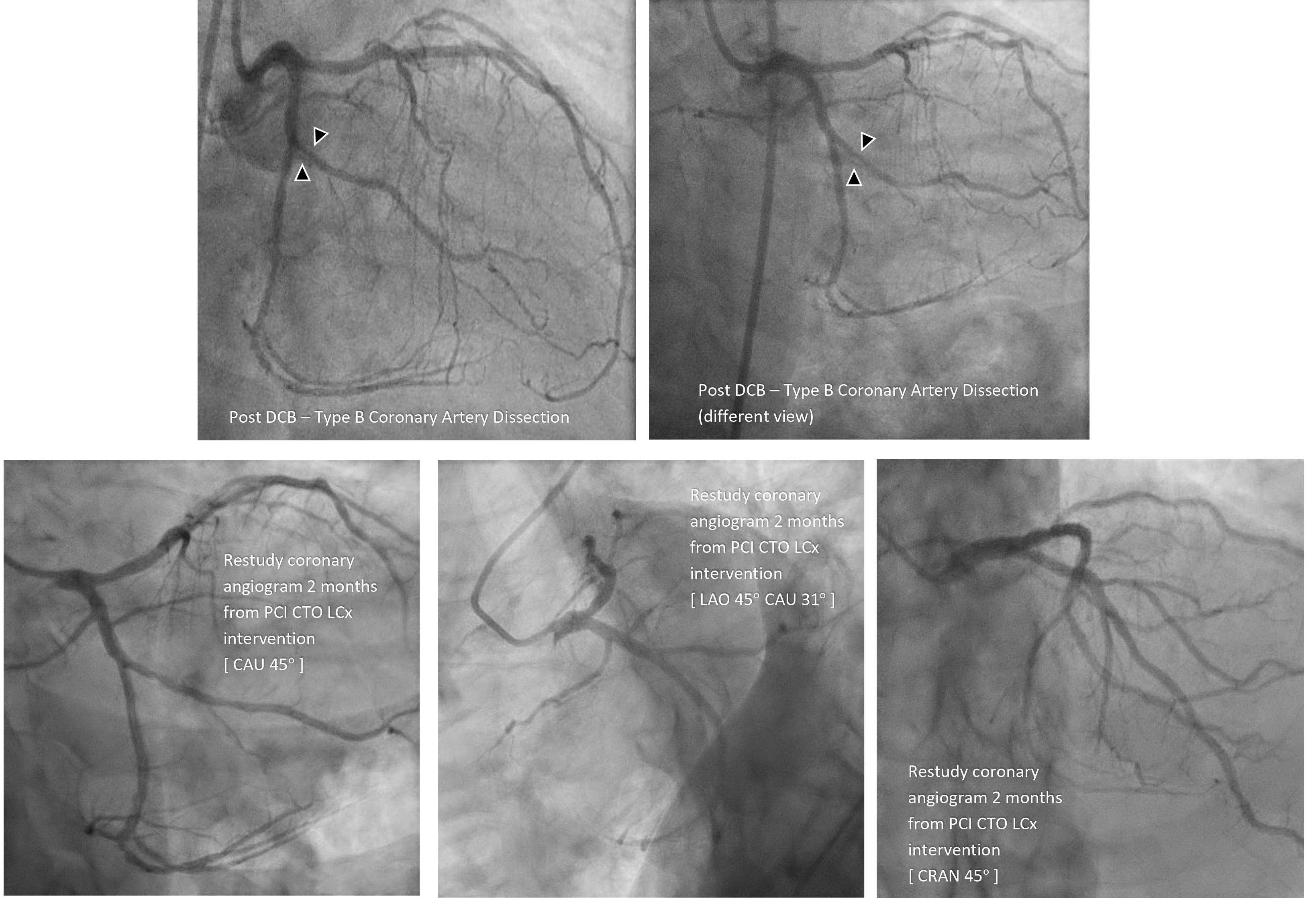
During index coronary angiogram, EBU 3.5 6Fr was used to engage the left system. Attempt was made to cross CTO LCx with Sion blue, Fielder XT and Finecross with subsequent parallel wiring technique using dual lumen catheter (Crusade). However, failed to enter true lumen distally. Procedure abandoned. No complications. Reattempt PCI to CTO LCx was performed 2 months later. J-CTO score was 3. Similar guide catheter was used as before. Wired down LCx with Fielder XT-A and microcatheter (Caravel). Able to cross lesion. Subsequently exchanged to Turnpike Spiral Catheter and able to advance across the CTO. Predilatation with Accuforce 2.5/15mm till 12 atm. Able to wire further into distal part of the 3rd Om branch. Exchanged to Runthrough Floppy workhorse wire. Wired down 2nd Om branch with Sion blue and predilated with Ryurei 1.5/15mm till 14atm, Ryurei 2.0/15mm till 12atm and then NC Emerge 2.5/15mm till 12 atm. TIMI III flow established. Noted Type B dissection over proximal 2nd Om branch but non flow limiting. Proceeded with three drug coated balloons (Sequent Please Neo) 2.25/40mm at distal LCx, 2.5/20mm in 2nd Om branch followed by 2.5/40mm at mid segment of LCx. Given intracoronary nitroglycerin 100mcg X 2 bolus doses. Procedure paused and waited for 15 minutes. Repeated angiographic shot showed TIMI III flow with Type B dissection which was non flow limiting. Results accepted.
Restudy coronary angiogram 10 weeks later, dissection has healed well with good TIMI III flow in LCx.
Restudy coronary angiogram 10 weeks later, dissection has healed well with good TIMI III flow in LCx.
Case Summary
CTOs remain a challenge to many operators. Reattempt via antegrade approach can be difficult but with the right usage of microcatheter such as Turnpike Spiral catheter, crossing the lesion and advancing wires can be made easier. Treatment of lesion with drug coated balloons (DCB) especially in CTOs have been well studied and was used extensively in this case. Despite complication of non-flow limiting coronary artery dissection, the vessel healed well during the restudy angiogram with no late lumen loss or target vessel failure. Therefore, it is feasible to use DCB in de novo CTOs and this case demonstrated the safety of leaving a dissection after DCB angioplasty.