
Lots of interesting abstracts and cases were submitted for TCTAP 2022. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-162
Severe Hand Hematoma Sparing the Forearm Post Percutaneous Coronary Intervention via Distal Radial Artery
By Mohd Asyiq Al-Fard Bin Mohd Raffali, Shawal Faizal Mohamad, Noor Diyana Binti Mohamad Farouk, Hamat Hamdi Che Hassan
Presenter
Mohd Asyiq Al-Fard Bin Mohd Raffali
Authors
Mohd Asyiq Al-Fard Bin Mohd Raffali1, Shawal Faizal Mohamad1, Noor Diyana Binti Mohamad Farouk1, Hamat Hamdi Che Hassan1
Affiliation
Hospital Canselor Tuanku Muhriz UKM, Malaysia1,
View Study Report
TCTAP C-162
OTHERS - Vascular Access (Transradial)
Severe Hand Hematoma Sparing the Forearm Post Percutaneous Coronary Intervention via Distal Radial Artery
Mohd Asyiq Al-Fard Bin Mohd Raffali1, Shawal Faizal Mohamad1, Noor Diyana Binti Mohamad Farouk1, Hamat Hamdi Che Hassan1
Hospital Canselor Tuanku Muhriz UKM, Malaysia1,
Clinical Information
Patient initials or Identifier Number
JM
Relevant Clinical History and Physical Exam
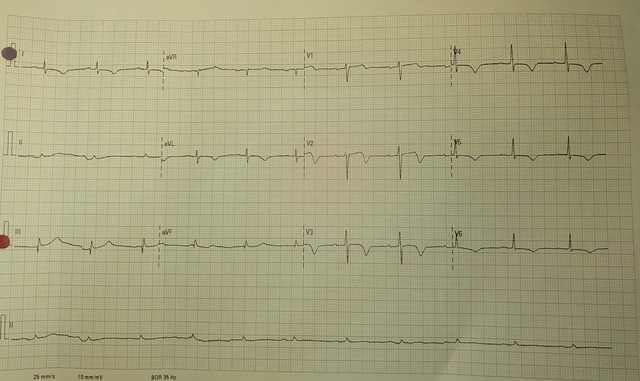
A 65-year-old gentleman presented to our emergency department for acute chest pain in the morning. Upon arrival, he was alert but diaphoretic. His blood pressure was 135/70 mm Hg with heart rate of 90 beats per minute. Electrocardiogram showed widespread bifid T over the precordial leads suggestive of Wellens syndrome.
Relevant Test Results Prior to Catheterization
High sensitivity cardiac troponin-I was elevated, and serial ECG showed dynamic changes.
Relevant Catheterization Findings
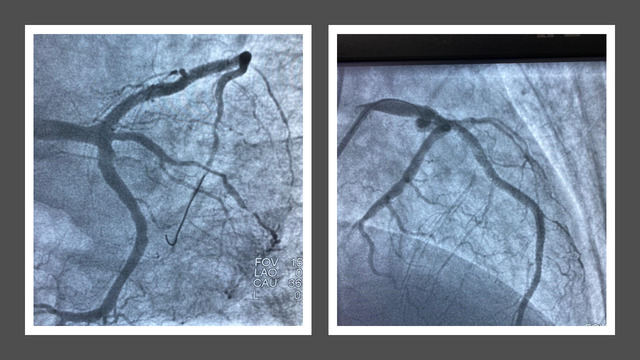
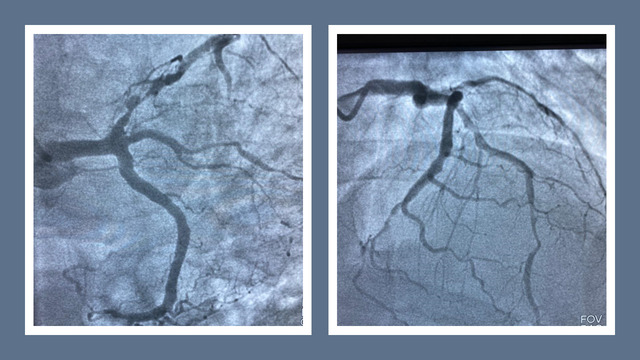
Patient proceeded with coronary angiography for high risk NSTEMI via right distal transradial access. Patient was found to have three vessel disease with subtotal occlusion of the proximal LAD and proceeded with stenting over the culprit lesion without any complication.
Interventional Management
Procedural Step
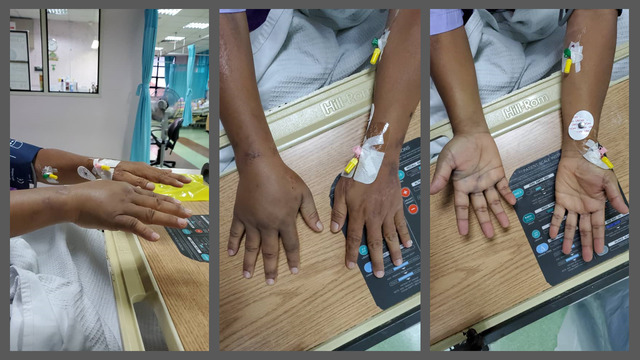
Throughout the procedure, the patient was administered with 11,000 unit of intraarterial unfractionated heparin, and oral ticagrelor 180 mg stat. No hematoma over the access site, and the radial sheath was removed with manual compression of about 10 minutes, and compression bandaging was applied. Upon returning to the ward, the patient complained of extensive right-hand swelling with pain and numbness. The patient was immediately attended by the on-call resident. On examination, the whole hand was swollen over both palmar and dorsal region, amazingly the hematoma didn’t extend proximally beyond the wrist. Proximal radial pulse was palpable, capillary refill time was less than 2 seconds, and color was still pink. Manual compression was continued for an hour with the right upper limb placed on elevated position and ice compression applied afterwards.
 post removal2.jpg
post removal2.jpg

post removal.jpg

preremoval.jpg
Case Summary
After prolonged compression, the hematoma stopped expanding further. The next morning, the hematoma slowly regressed, and an orthopedic consultation was made to review the hand, in which no features of compartment syndrome at the time. The next day, the patient was discharged uneventfully, with partial resolution of the hand hematoma. Formation of hand hematoma post distal radial artery catheterization should be taken seriously as risk of compartment syndrome is possible due to its anatomical features. Immediate measures must be taken to prevent hematoma expansion, and early orthopedic consultation is warranted if fasciotomy is indicated.