
Lots of interesting abstracts and cases were submitted for TCTAP 2022. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-014
Successful Transradial Percutaneous Coronary Intervention in Dextrocardia
By Suhashni Gnaneswaran, Seong Kooi Khaw, Houng Bang Liew
Presenter
Suhashni Gnaneswaran
Authors
Suhashni Gnaneswaran1, Seong Kooi Khaw1, Houng Bang Liew2
Affiliation
Hospital Queen Elizabeth II, Malaysia1, Queen Elizabeth II Hospital, Malaysia2,
View Study Report
TCTAP C-014
CORONARY - Acute Coronary Syndromes (STEMI, NSTE-ACS)
Successful Transradial Percutaneous Coronary Intervention in Dextrocardia
Suhashni Gnaneswaran1, Seong Kooi Khaw1, Houng Bang Liew2
Hospital Queen Elizabeth II, Malaysia1, Queen Elizabeth II Hospital, Malaysia2,
Clinical Information
Patient initials or Identifier Number
HH
Relevant Clinical History and Physical Exam
57 years old gentleman with underlying diabetes and hypertension had a history of anterior ST-elevation myocardial infarction in June 2021 for which he had received successful thrombolytic therapy.He was subsequently referred to our Cardiology centre from one of our referring periphery hospitals and was scheduled for an elective angiogram in November 2021.He was asymptomatic and physical examination was unremarkable except for findings consistent with dextrocardia and palpable liver on left side.
Relevant Test Results Prior to Catheterization
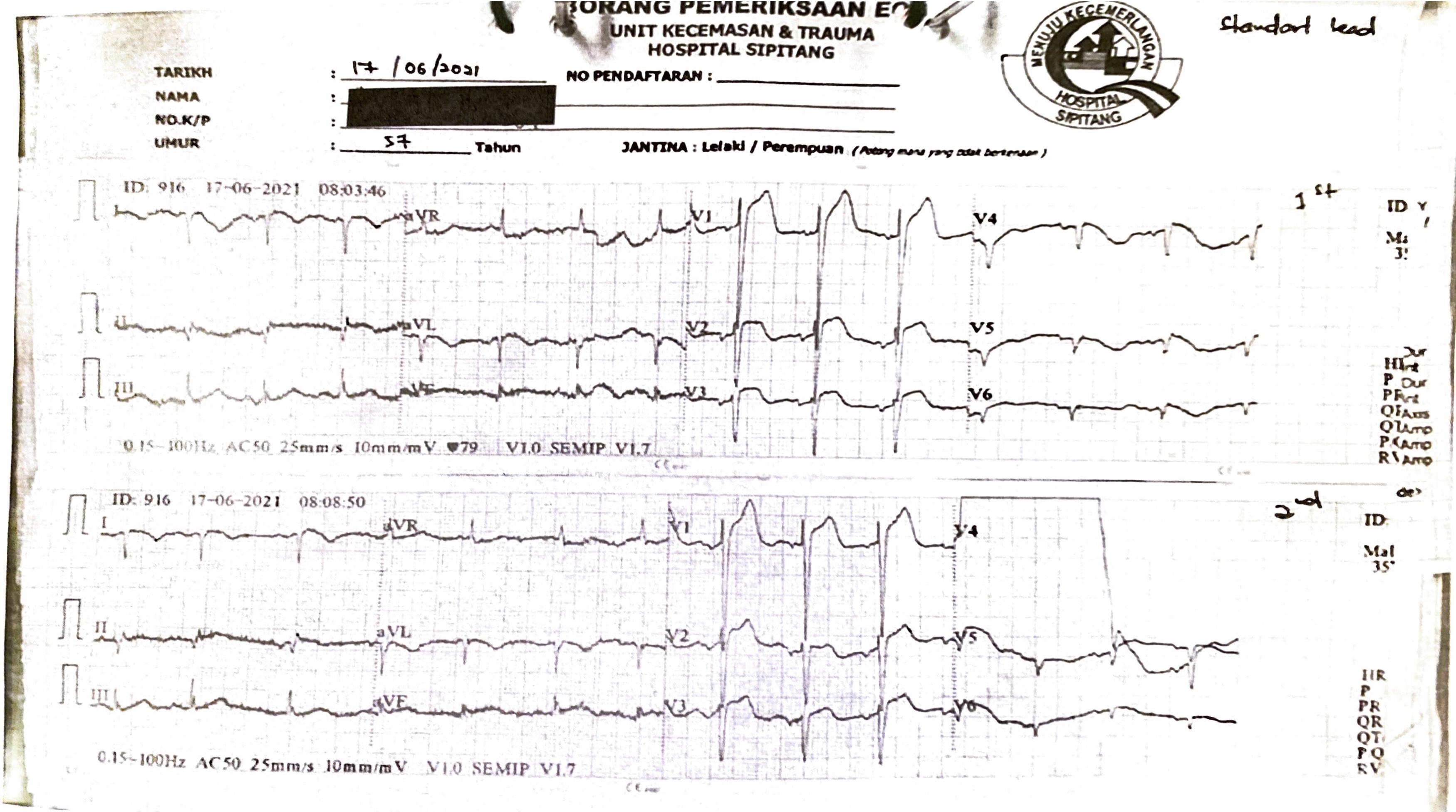
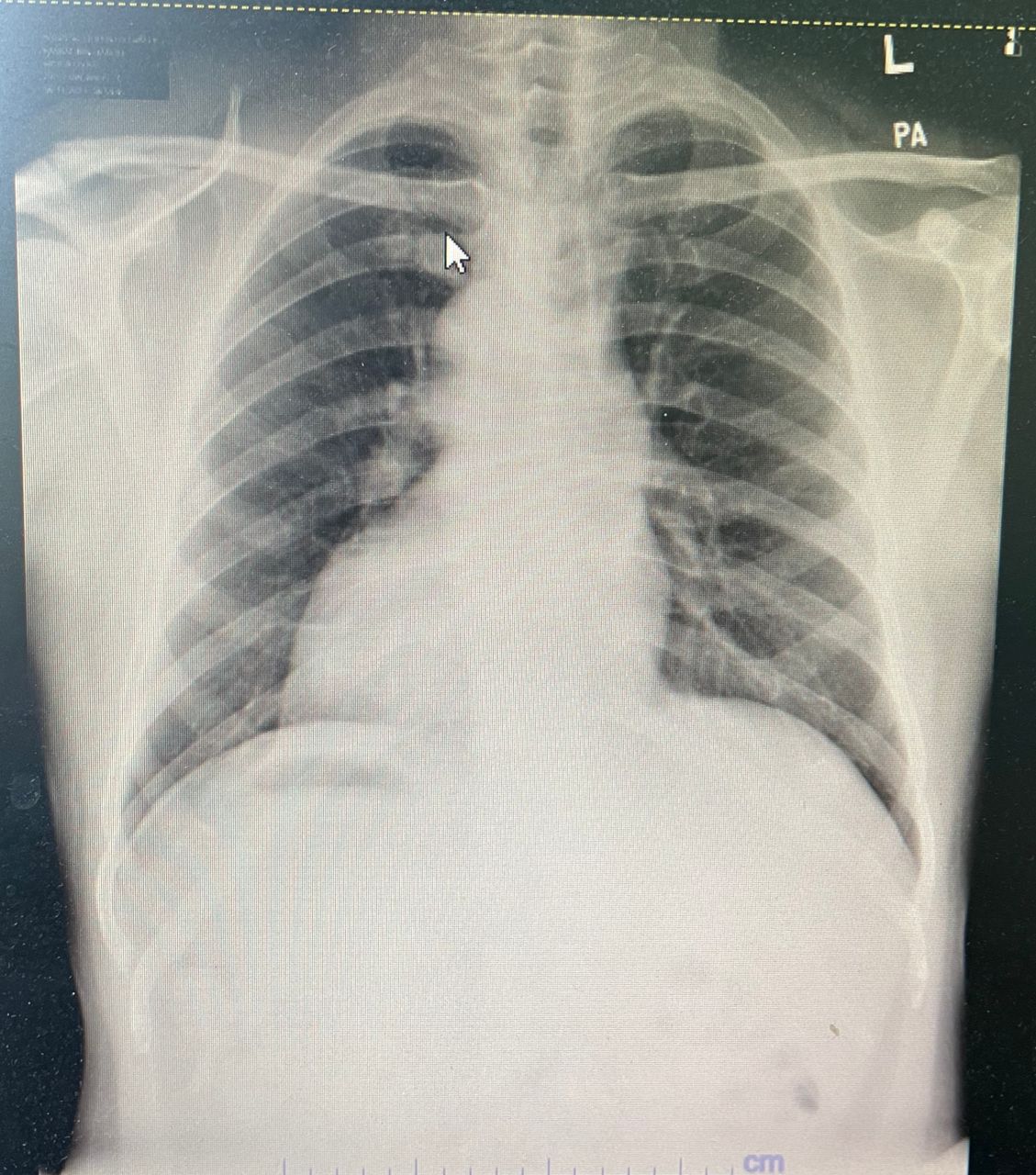
Initial ECGs with usual placement of the electrodes taken during the acute episode at casualty in June 2021 showed sinus rhythm with right axis deviation, ST elevation in anterior leads with positive QRS complexes (upright P and T waves) in aVR.Lead 1 and aVL showed global negativity (inverted P wave, negative QRS, inverted T wave). Absent R wave progression in chest leads. Chest x-ray showed the apex of the heart and gastric bubble to the right which adds to the diagnosis of situs inversus.
Relevant Catheterization Findings
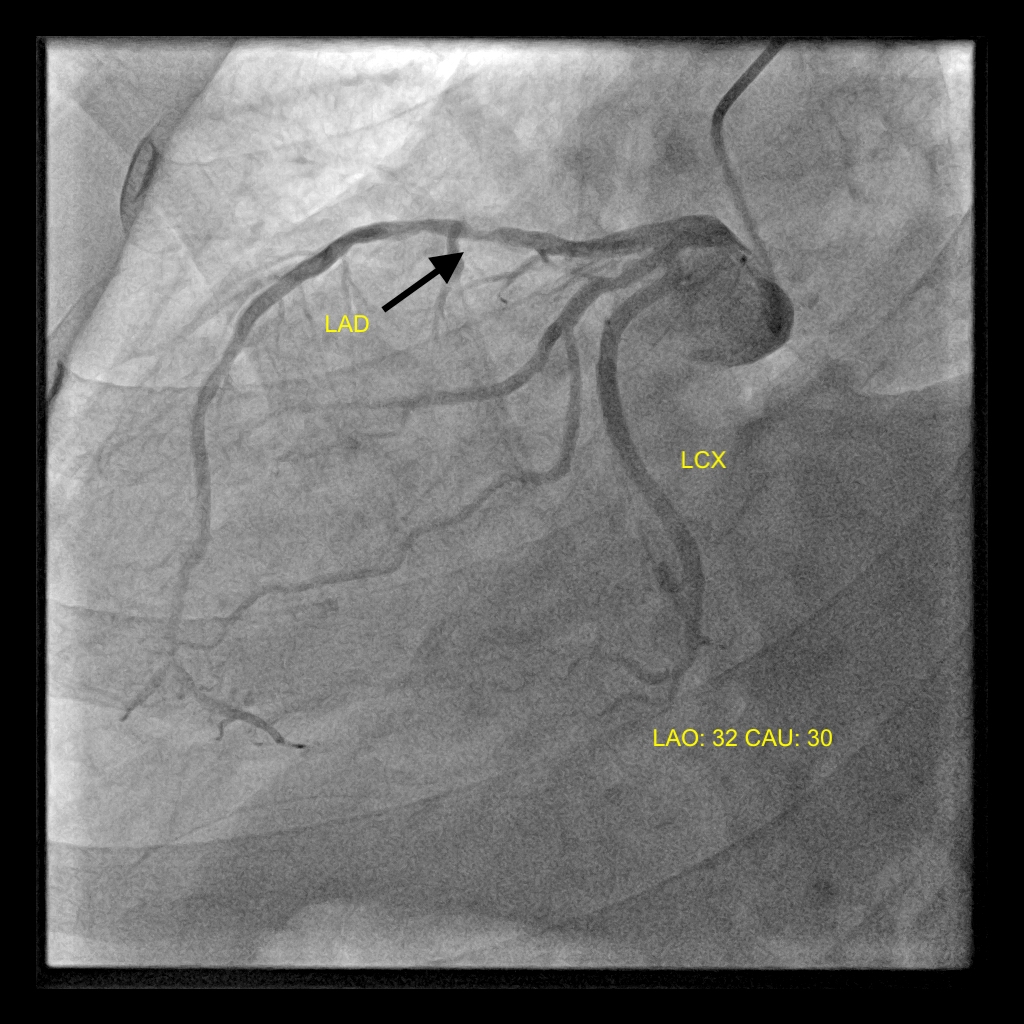
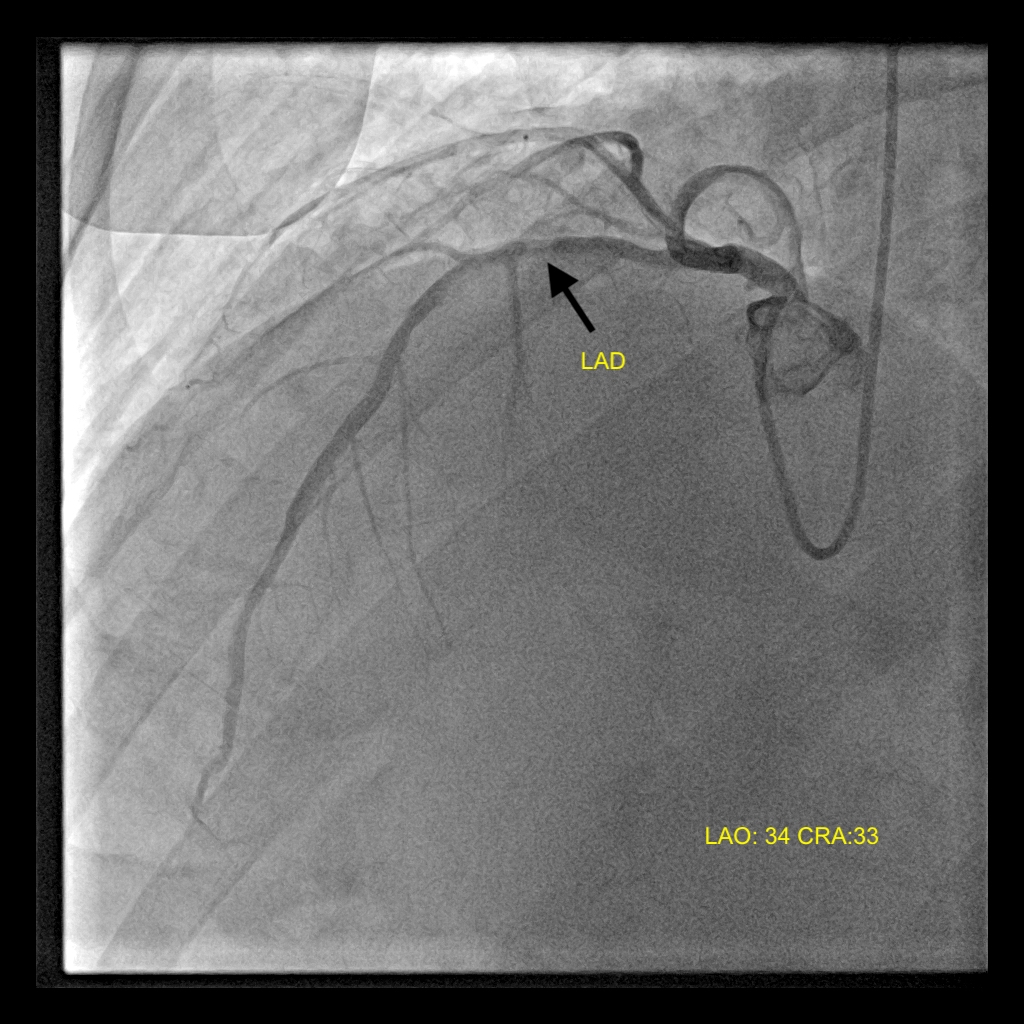
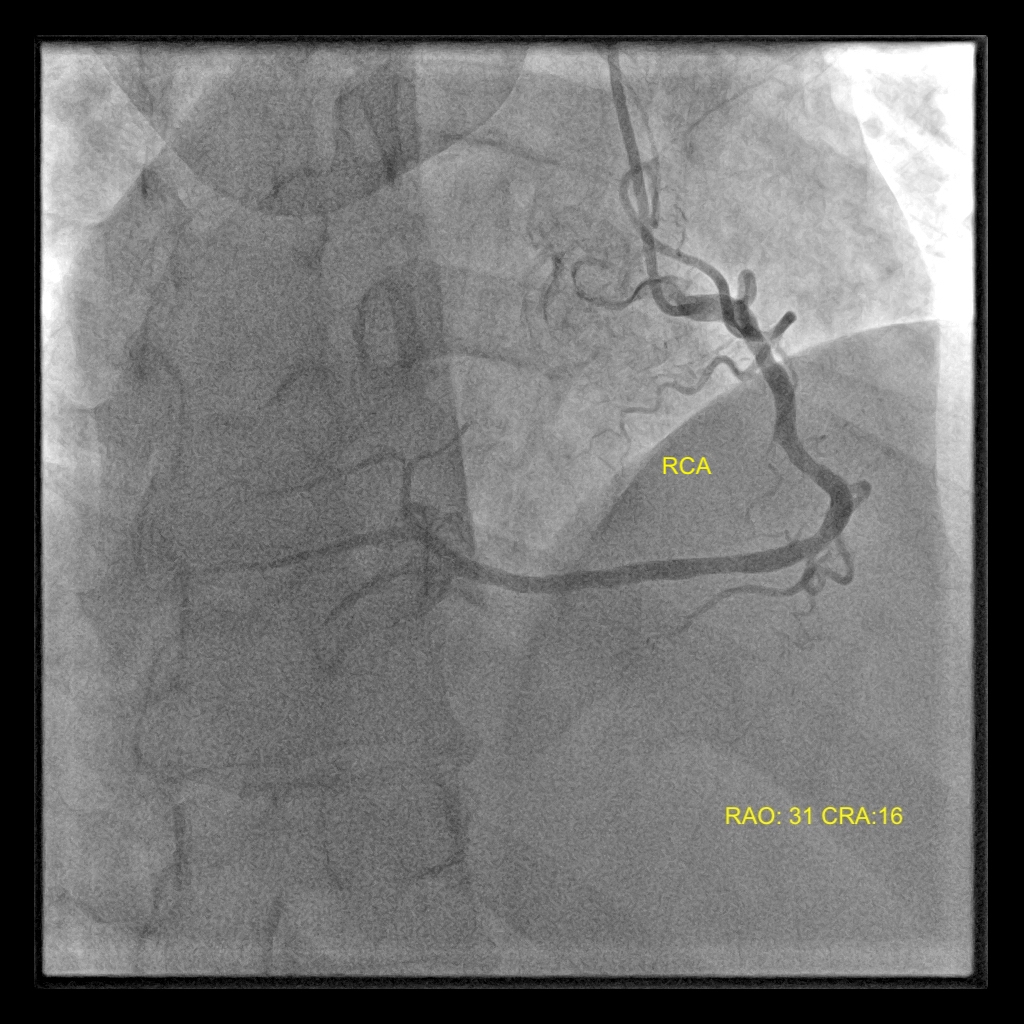
Diagnostic coronary angiography revealed single vessel disease with proximal left anterior descending artery (LAD) discrete lesion 70-80%; TIMI grade 3 flow. The left main stem (LMS) and left circumflex (LCX) was normal. The right coronary artery (RCA) was dominant with normal findings as well.
Interventional Management
Procedural Step
Under local anaesthesia, right radial artery was punctured.A 6 French(Fr) radial sheet was inserted. Diagnostic coronary angiography performed with a 5Fr Terumo Optitorque catheter.Selective engagement of left and right coronary arteries done in anteroposterior(AP) view. Multiview angiography performed with hand injection of contrast.
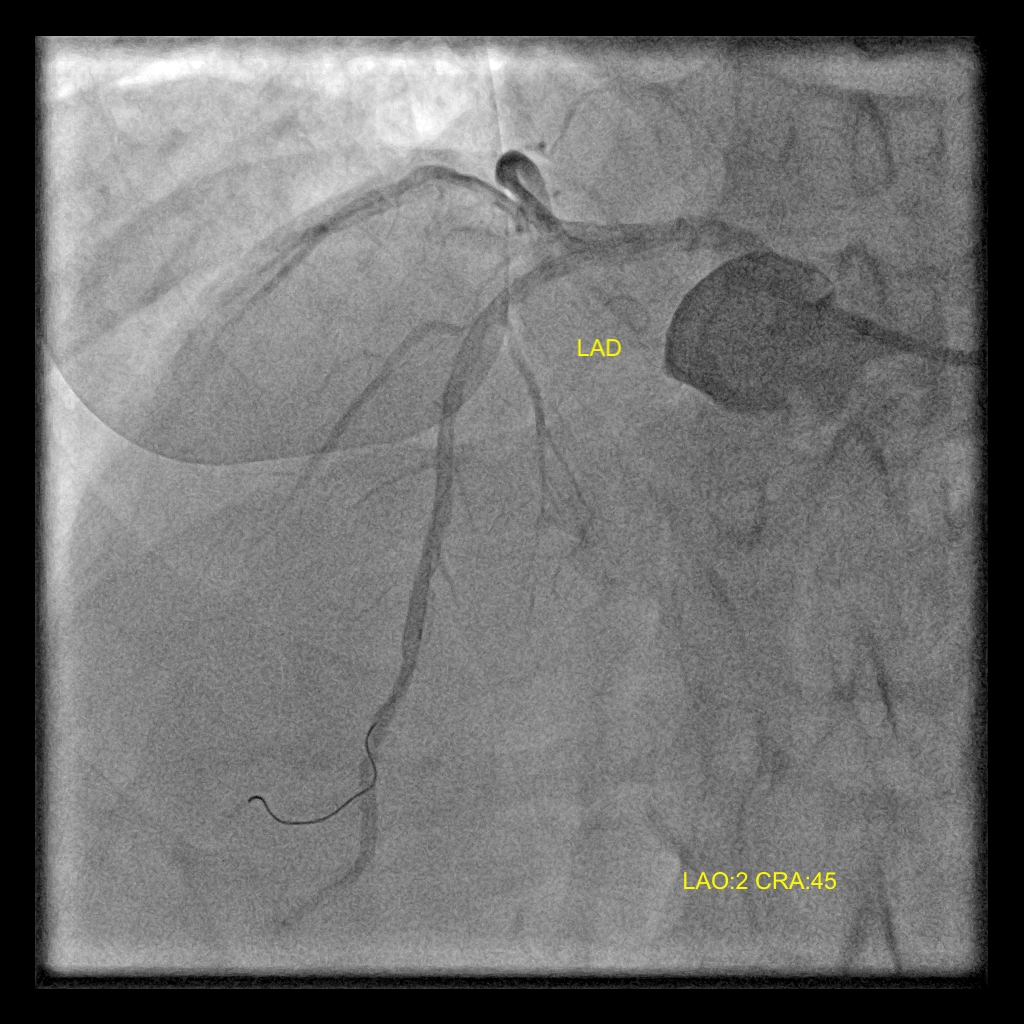
Proceeded with ad hoc percutaneous coronary intervention (PCI) to left anterior descending artery (LAD).A 6Fr extra-backup support(EBU) 3.0 guiding catheter was used to engage the left coronary artery in AP view. A Balance Middleweight(BMW) guide wire was passed into the LAD.The proximal LAD lesion was pre-dilated with a semi compliant(SC) Sprinter Legend balloon 3.5mmx12mm. Post pre-dilatation, no significant dissection or recoil was noted.Thus, decision was made to treat the proximal LAD lesion with Drug Eluting Balloon (DEB) Sequent Please Neo 3.5mmx20mm at 6atm for 60 seconds.
Post DEB, there was excellent angiographic results with minimal recoil and TIMI grade 3 flow.
Post procedure, the radial sheath was removed. Nichiban was applied and homeostasis was secured.
Patient was transferred to our cardiac recovery ward and was observed over 24 hours and subsequently discharged home.
Case Summary
In the case reported here, we demonstrate that the coronary interventional management of individuals with dextrocardia follows the same general rules as for non-dextrocardia patients but some technical details should be taken into consideration.
We performed the PCI via radial approach.Standard catheters can be used but their manipulation must be in the opposite direction.We simply used equivalent right sided views to produce the usual left sided images and vice versa.Hence the image intensifier in the LAO cranial position yielded a mirror image of the RAO cranial view.Once images were obtained, we performed angioplasty to LAD with standard wires and balloons with excellent angiographic outcome.