
Lots of interesting abstracts and cases were submitted for TCTAP 2022. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-142
Back to Basic "History Taking"
By Glendon Seng Lau, Surasee Srihasarn, Panat Nisityotakul, Keerati Hongsakul
Presenter
Glendon Seng Lau
Authors
Glendon Seng Lau1, Surasee Srihasarn2, Panat Nisityotakul2, Keerati Hongsakul2
Affiliation
Hospital Sultan Idris Shah Serdang, Malaysia1, Prince of Songkla University, Thailand2,
View Study Report
TCTAP C-142
ENDOVASCULAR - Peripheral Vascular Disease and Intervention
Back to Basic "History Taking"
Glendon Seng Lau1, Surasee Srihasarn2, Panat Nisityotakul2, Keerati Hongsakul2
Hospital Sultan Idris Shah Serdang, Malaysia1, Prince of Songkla University, Thailand2,
Clinical Information
Patient initials or Identifier Number
1984031
Relevant Clinical History and Physical Exam
84 years old male
Chronic smoker Presented in November 2015 with both leg claudication for 3 months and ulcer over left ankle.Pulses over left limb weak .Angiogram and stented both CIA in November 2015 .Review March 2016 with CTA -symptoms persist, plan for medication.Pain worsen, repeat angiogram July 2016- stented bilateral CIA with BE and SE.Review August 2016 with CTA July 2016, pain persist, offered history of abdominal massage with coconut. Angiogram October 2016-stent both CIA with SE stent
Chronic smoker Presented in November 2015 with both leg claudication for 3 months and ulcer over left ankle.Pulses over left limb weak .Angiogram and stented both CIA in November 2015 .Review March 2016 with CTA -symptoms persist, plan for medication.Pain worsen, repeat angiogram July 2016- stented bilateral CIA with BE and SE.Review August 2016 with CTA July 2016, pain persist, offered history of abdominal massage with coconut. Angiogram October 2016-stent both CIA with SE stent
Relevant Test Results Prior to Catheterization
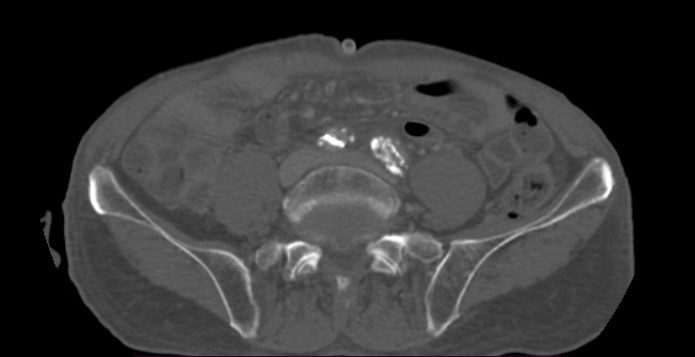
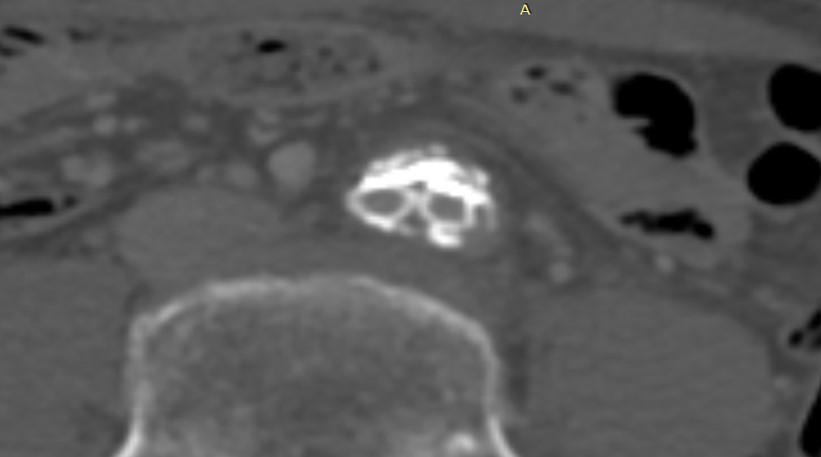
Investigations - no significant abnormalities ( Renal, liver and lipid profile , HbA1C and full blood counts within normal range )CTA October 2015 -severe atherosclerosis at left external iliac artery and distal left superficial femoral artery to popliteal artery .Repeated CTA March 2016- shows nearly complete collapse of bilateral common iliac artery stent . CTA July 2016 after procedure shows restenosis of stent particularly the BE stent sparing the SE stent.CTA in January 2017- patent stent
Relevant Catheterization Findings
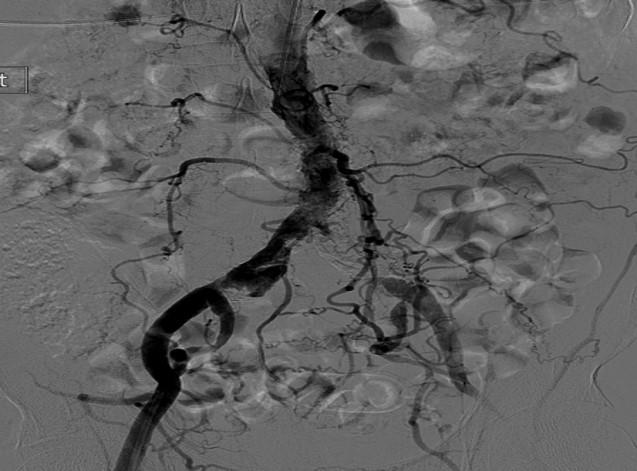
Diagnostic Angiogram during first PTA November 2015 - severe stenosis over left CIA , moderate stenosis over right CIA Repeated Angiogram ( second PTA ) July 2016 shows in stent re- stenosis of bilateral CIA .
Interventional Management
Procedural Step
First angiogram ( November 2015) .


Antegrade approach via left brachial , retrograde via bilateral femoral artery .
Wired with terumo 0.35, exchange to Advantage 0.35 .
Predilated bilateral CIA with kissing balloon , Right CIA with Juturna 0.35, 5mm x 60mm , Left CIA with Juturna 5mmx80mm .
Stented Right CIA with Omnilink 8mmx39mm and Dynamic 8mmx38mm , stented left CIA with Dynamic 8mmx56 mm.
Completed with kissing balloon with stent balloon at bilateral CIA.
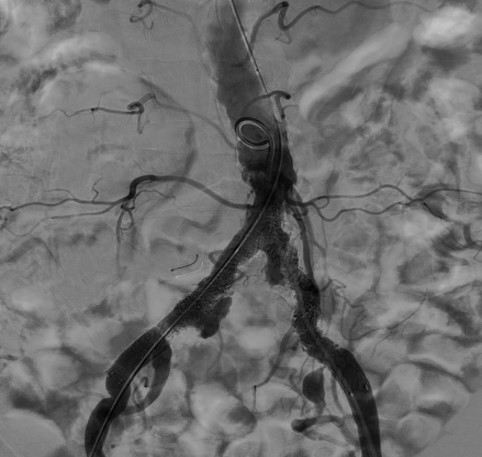
Second angiogram ( July 2016) .
Retrograde approach via bilateral femoral .
Wired with terumo 0.35, exchange to advantage 0.35 .
Predilated both CIA stents ( total collapsed segment) with Passeo 6mmx80mm .
stented Right CIA with Omnilink 7mmx59mm and Astron 8mmx40mm ( proximally) .
stented left CIA with express LD 7mmx 57mm and Smart flex 8mm x 40mm ( proximally).
completed with kissing balloon with stent balloon at bilateral CIA.
Final Angiogram ( October 2016).
Retrograde approach via bilateral femoral.
Wired with terumo , exchange wire to supracore bilaterally.
Initially predilated both CIA with Passeo 5mmx60mm , than upsized to Armada 35, 7mmx60mm bilateral CIA .
Opted for self expandable stent , stented Right CIA with Abott Absolute pro 7mmx60mm , similarly Left CIA was stented with Abott Absolute pro 7mmx60mm
Repeated CTA January 2017 - patent bilateral CIA stents .patient was asymptomatic and was discharged back to referring hospital.
Case Summary
Patient was discharge well after the last procedure, repeated CTA shows patent Bilateral CIA stents and patients remains asymptomatic. This case just illustrate to us not to neglect basic history taking. To date there is lack of comparative data between self expanding stents( SE ) and balloon expandable stent ( BE) in treatment of iliac artery occlusive disease . In our case we notice that the restenosis occurred in the distal segment of CIA stented with BE sparing the segment stented with SE. The randomized ICE trial did show lower rate of restenosis and significantly lower TLR in SE as compared with BE at 12 months duration, however more data/ trial is needed.