
Lots of interesting abstracts and cases were submitted for TCTAP 2022. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-161
Vasospastic Angina With Life-Threatening Arrhythmia: To Implant or Not to Implant; That Is the Question
By Zainab Dakhil, Mahmoud AlHaleem, Muthanna AlQuraishi
Presenter
Zainab Dakhil
Authors
Zainab Dakhil1, Mahmoud AlHaleem2, Muthanna AlQuraishi2
Affiliation
Ibn Al-Bitar Hospital, Iraq1, Ibn Al-Bitar Centre, Iraq2,
View Study Report
TCTAP C-161
OTHERS - Quality, Guidelines and Appropriateness Criteria
Vasospastic Angina With Life-Threatening Arrhythmia: To Implant or Not to Implant; That Is the Question
Zainab Dakhil1, Mahmoud AlHaleem2, Muthanna AlQuraishi2
Ibn Al-Bitar Hospital, Iraq1, Ibn Al-Bitar Centre, Iraq2,
Clinical Information
Patient initials or Identifier Number
G.S.KH
Relevant Clinical History and Physical Exam
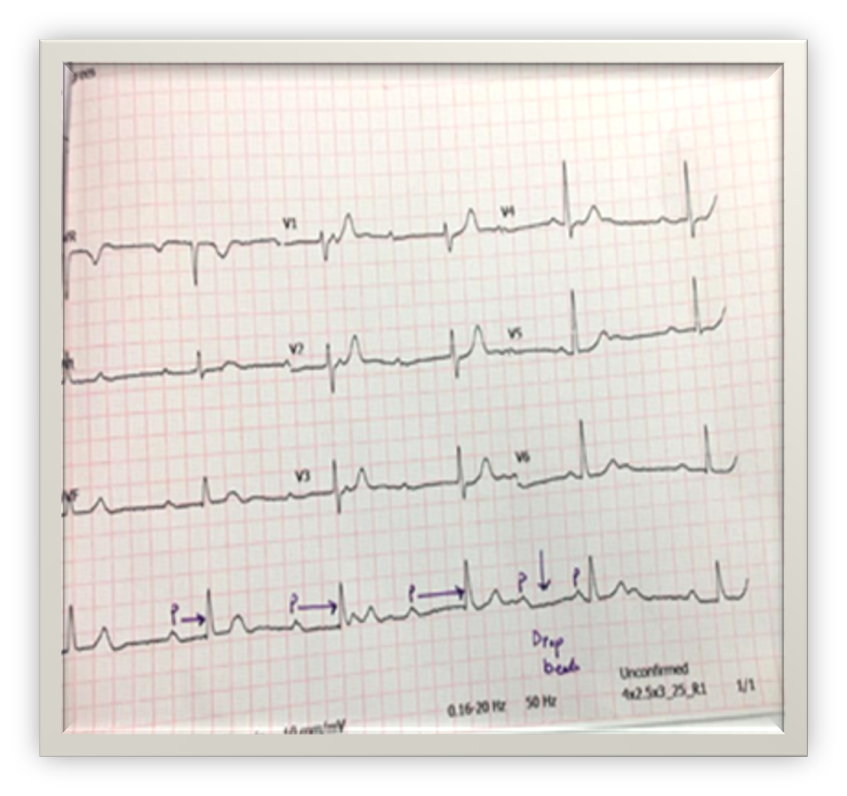
A 65-year-old hypertensive smoker male presented to general hospital as sudden cardiac arrest, he was resuscitated successfully there, his ECG there showed Complete Heart Block (CHB) so he was referred to our cardiac center where he reported severe central chest pain.
Relevant Test Results Prior to Catheterization
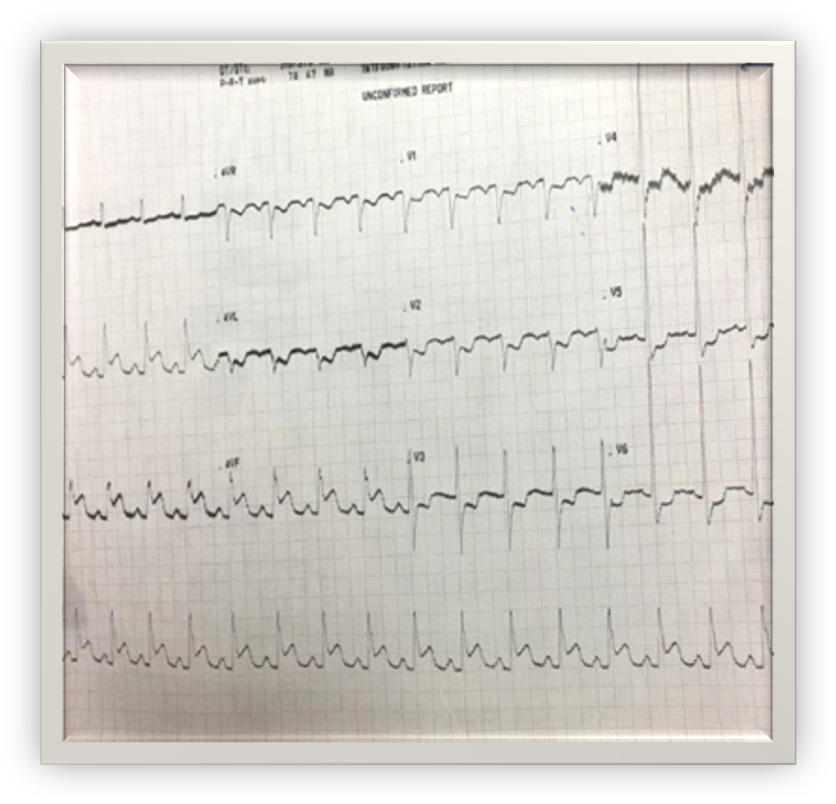
His Electrocardiogram at our centre revealed ST elevation in inferior leads.His troponin test was positive (Qualitative assay).His Echocardiography revealed anteroseptal hypokinesia, good LV systolic function.
Relevant Catheterization Findings
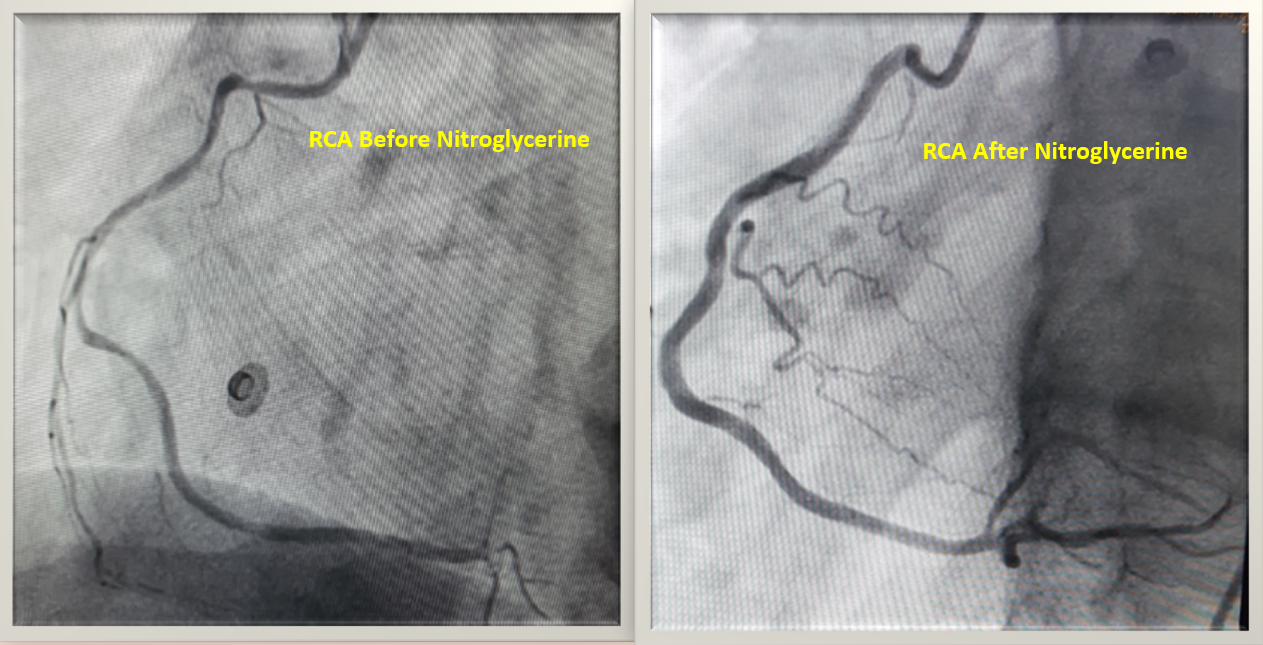
Immediate Coronary angiography showed: Mid bifurcational LAD intermediate lesion, diffusely small RCA.We suspected coronary artery vasospasm so intracoronary nitroglycerine was given, then we repeated right coronary angiography which showed: normal RCA.After 2 hours in the CCU he had VT/VF and resuscitated successfully, so taken back to the catheterisation lab where second coronary angiography was done and showed RCA vasospasm with no complication from earlier procedure.
Interventional Management
Procedural Step
Then patient was transferred to CCU and kept on intravenous nitroglycerine, oral calcium channel blocker (CCB) (Amlodipine tab 5 mg) and nitrate (Isosorbide dinitrate 30 mg/day), he responded well with resolution of ECG changes (ST elevation), restoration of normal heart rate (93 bpm) with no evidence of heart block. At 3rd day in CCU he had rapid Atrial Fibrillation that treated by IV CCB (Verapamil), so regained sinus rhythm, we used maximum tolerated doses of oral CCB and nitrate.The cardiac team was conflicting regarding the decision to implant or not an ICD for this patients who had sudden cardiac arrest in the context of vasospastic angina (VSA).In the context of VSA and ventricular arrhythmia and according to ACC guideline: it is class I indication to start CCB. It is a class IIa indication for ICD implantation for VSA that presented with Sudden cardiac death (SCD) if optimal medical therapy (OMT) was ineffective while in a patient like ours; it is a class IIb to implant ICD along with OMT for VSA if presented with SCD without waiting to determine response to OMT. Accordingly, the heart team opted out ICD implantation and chose to keep him on OMT with close follow up, he was also instructed to quit smoking then he was discharged well. At 1-,4-, 6-and 12 months follow-up the patient denied any further episodes of palpitation, presyncope or syncope.
Case Summary
VSA is a functional coronary artery disease that receives more attention recently, despite the favorable prognosis it is a well-recognized trigger for lethal ventricular arrhythmia; a setting when literature is debatable regarding which patient needs to have ICD in addition to optimal medical therapy.
Evidence-based OMT can be used in VSA with ventricular arrhythmia and can omit the need for ICD implantation. Future studies are warranted to risk stratify patients with vasospastic angina who presented with ventricular arrhythmia and to assess the outcomes of different treatment strategies especially in Asian population in whom this coronary entity is more common compared to other populations.
Evidence-based OMT can be used in VSA with ventricular arrhythmia and can omit the need for ICD implantation. Future studies are warranted to risk stratify patients with vasospastic angina who presented with ventricular arrhythmia and to assess the outcomes of different treatment strategies especially in Asian population in whom this coronary entity is more common compared to other populations.