
Lots of interesting abstracts and cases were submitted for TCTAP 2022. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-170
VSR With Cardiogenic Shock
By Thanawat Suesat
Presenter
Thanawat Suesat
Authors
Thanawat Suesat1
Affiliation
Khon Kaen Hospital, Thailand1,
View Study Report
TCTAP C-170
STRUCTURAL HEART DISEASE - Others (Structural Heart Disease)
VSR With Cardiogenic Shock
Thanawat Suesat1
Khon Kaen Hospital, Thailand1,
Clinical Information
Patient initials or Identifier Number
J N
Relevant Clinical History and Physical Exam
50 year old Thai FemaleCC : dyspnea for 1 day PI : 3 day PTA chest pain off and on 1 day severe dyspnea with PND and orthopnea refer from local hospital PE : on ET tube BP 110 /70 mmHg RR 30 bpm HR 115 bpm PSM grade IV with thrill @ apex
 IMG_9187.MOV
IMG_9187.MOV
Relevant Test Results Prior to Catheterization
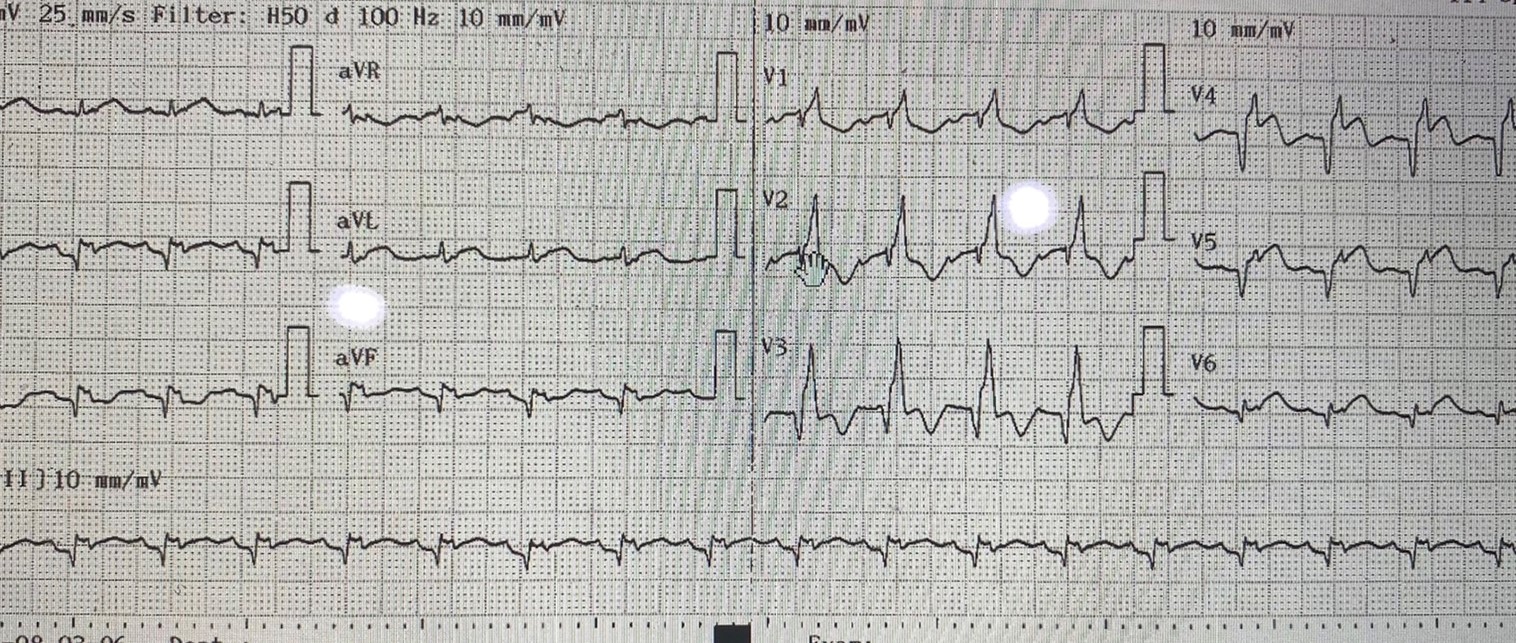
CXR pulmonary congestion echo : LVEF 50 % hypokinesia ant wall with VSR 1 cm antero- apical with left to right shunt Trop –T : 13,500
Dx : late STEMI with VSR with CHF
Dx : late STEMI with VSR with CHF
Relevant Catheterization Findings
LM: non sigficant stenosis LAD : 100 % occlusion mid LAD LCX : non sigficant stenosis RCA : 70 % pRCA LVEDP = 40 mmHg
2.avi
5.avi
7.avi
Interventional Management
Procedural Step
On IABP via RFA then consult CVT
IMG_9191.MOV
IMG_9190.MOV
18.avi
wait to 2 week for VSR repair + CABG Patient developed VT / acidosis / Cr rising (@ night )
BP drop required inotrope ,ECMO not available -
-> Consult nephrologist not stable for HD plan CRRT but intractable VT
Discussion with CVT + patient and relatives
plan POBA + transncatheter VSD closure + CVT standby
bridging for CABG and VSR repair
plan VSR closure via RFV
Trans femoral approach ( LFA + LFV)
LV gram show large VSR
JR 3.5 + Terumo wire cross from LV -->VSR -->RV --> RA --> IVC
snare to LFA created AV loop
Exchange to Amplatz supper stiff wire
gentle balloon sizing ( size = 12 mm ) with occlusion test
Cocoon ASD device size 20 mm was closed under
transthoracic echo guided
Small leakaged via Echo and LV gram
POBA to occlusion LAD but TIMI 1 flow
VT -- > improved
CHF -->improved
CRRT --> Cr and acidosis improved
Day 12
Echo show now leakage via VSR
CHF
CR rising
Day 14
CAVG + VSR repare
CHF -->improve
Cr --- > improve
Off ET tube 6 day after Sx
2 week later after Sx
pneumonia + sepsis
re intubation
AKI
CHF
againts advice
Case Summary
Ventricular septal defect(VSD) is a raremechanical complication of MI.Prognosis is very poorTranscatheter closure is a feasible andeffective alternative or bridging to surgery but still high mortality when closure during early day of infarction