
Lots of interesting abstracts and cases were submitted for TCTAP 2022. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-119
DCB Guided by Both OCT and FFR in the Treatment of ISR: A Case Report
By Wenduo Zhang
Presenter
Wenduo Zhang
Authors
Wenduo Zhang1
Affiliation
Beijing Hospital, China1,
View Study Report
TCTAP C-119
CORONARY - Drug-Eluting Balloons
DCB Guided by Both OCT and FFR in the Treatment of ISR: A Case Report
Wenduo Zhang1
Beijing Hospital, China1,
Clinical Information
Patient initials or Identifier Number
369241
Relevant Clinical History and Physical Exam
The male patient, 66 yrs, was implanted with three stents in m-dLAD(twice 2003&2010). DCB was performed for ISR in LAD stent in 2014. Recently, he was admitted to the hospital due to ACS one month (November 30, 2020). There were 2 years of type 20 diabetes, 20 years of hypertension, 10 years of hyperlipidemia, 10 years of hyperlipidemia, half a day of drinking and 3 smoking a day, denying family history. No obvious abnormality was found in physical examination.
Relevant Test Results Prior to Catheterization
Relevant Catheterization Findings
There is no obvious stenosis in LM, 25-50% stenosis in the proximal part of lad, isr25-50% in the original stent in the middle part of lad, 50-75% isr50-75% in the stent from the middle part of lad to the distal part, 50-75% stenosis in D1 opening, 50-75% diffuse stenosis in dlcx, 50-75% stenosis in OM1, 25-75% stenosis in pRCA, 25% stenosis in mRCA, 25% stenosis in dRCA, 75% stenosis in PDA,.
 CAGleft1.mp4
CAGleft1.mp4
CAGleft2.mp4
CAGleft3.mp4
cagleft4.mp4
CAGleft5.mp4
CAGRCA2.mp4
Interventional Management
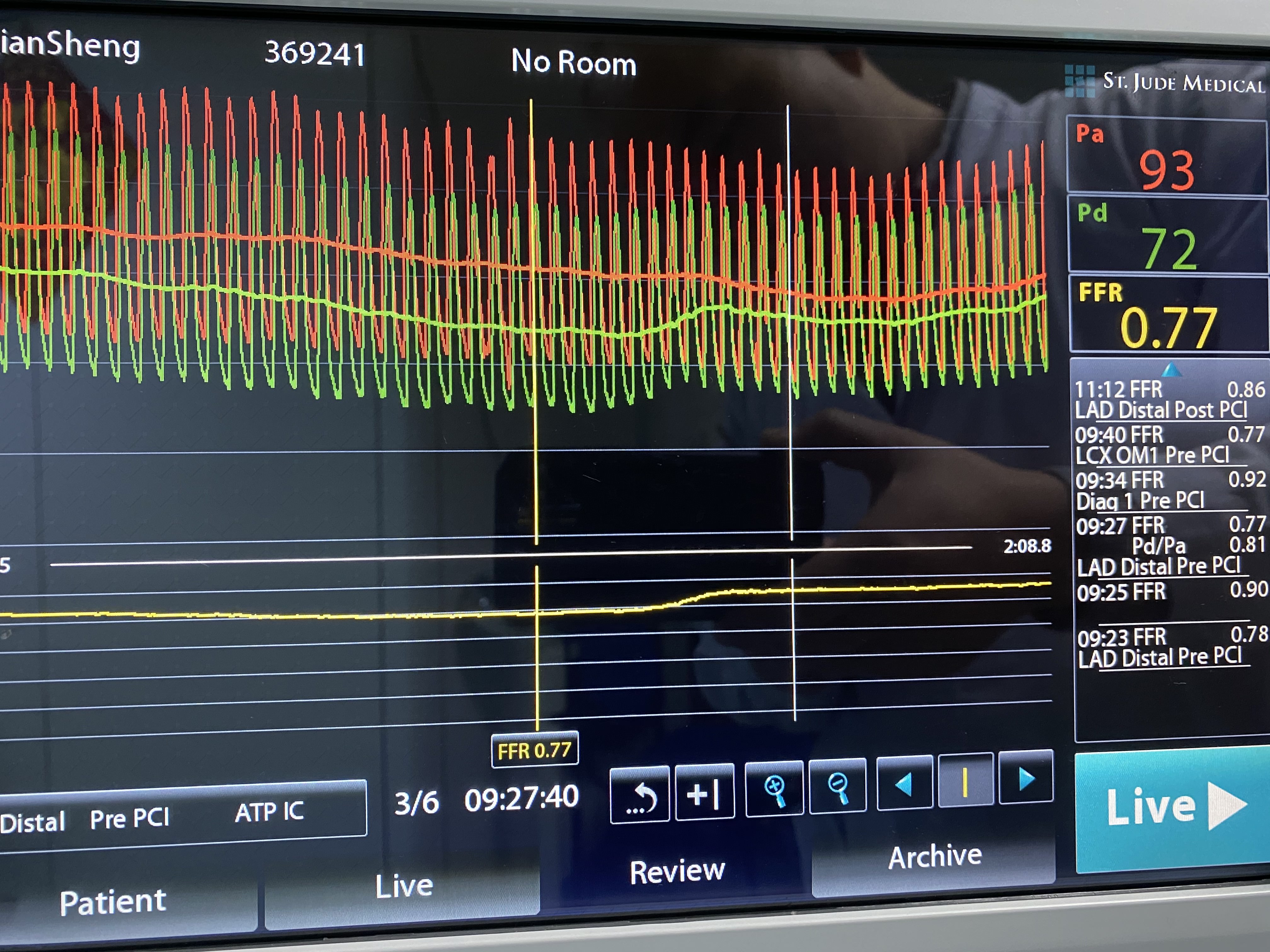
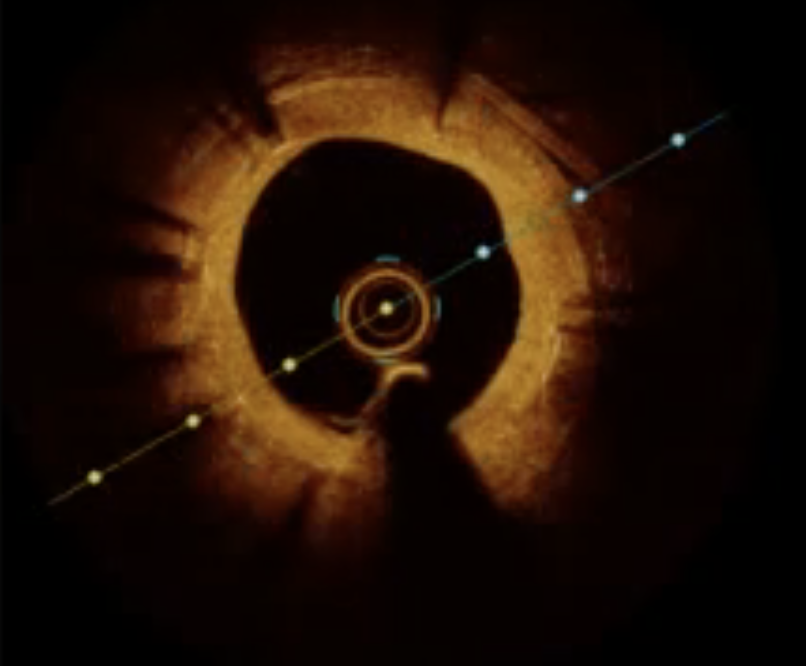
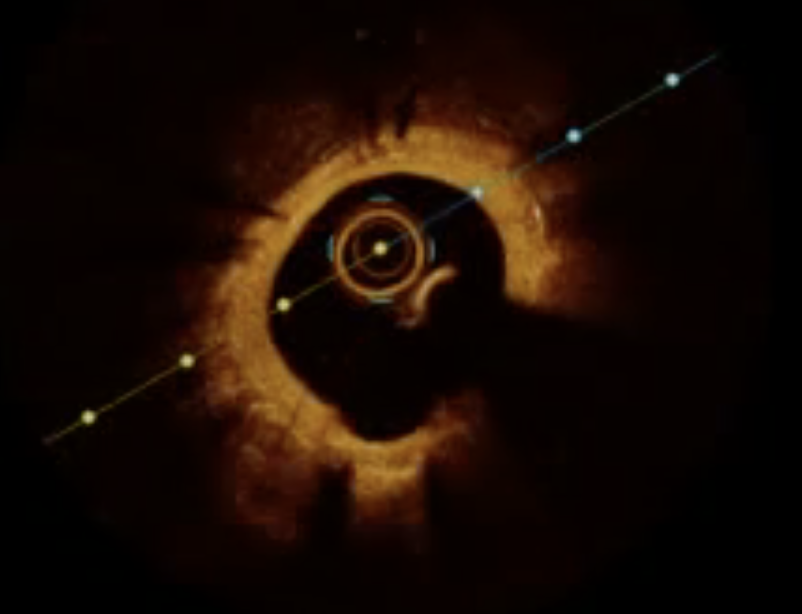
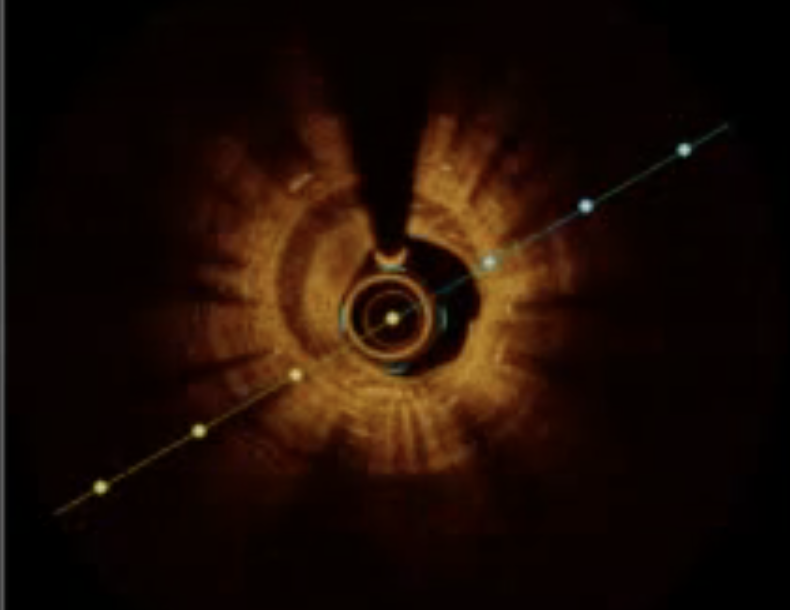
Procedural Step
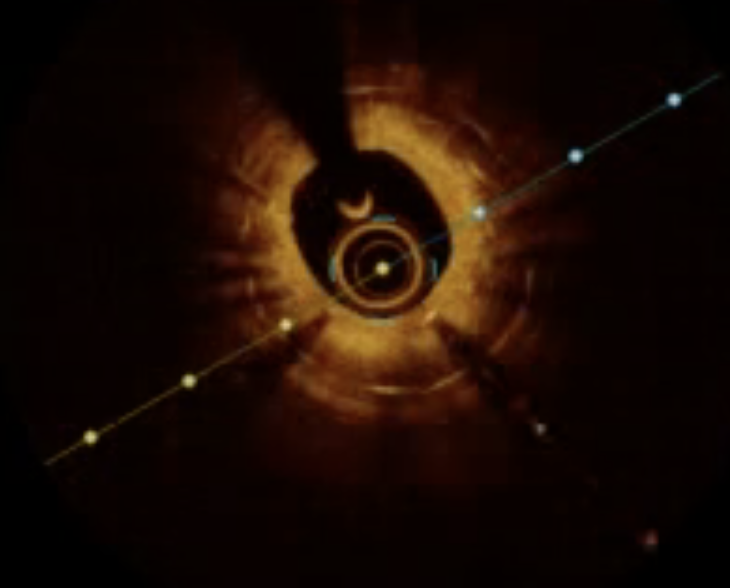
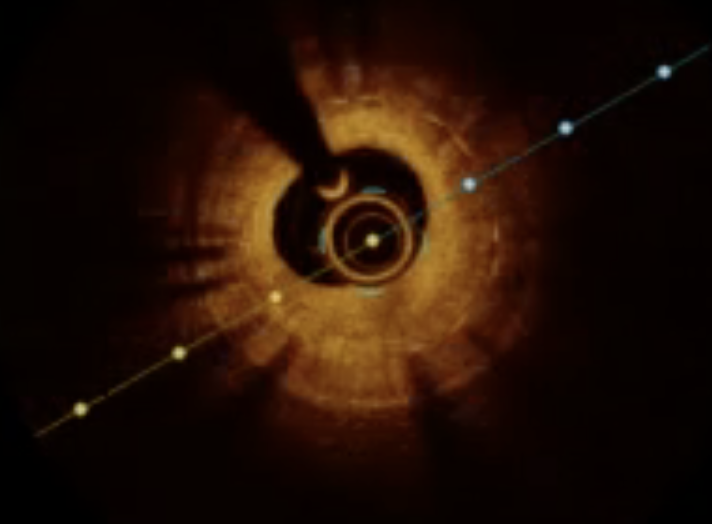
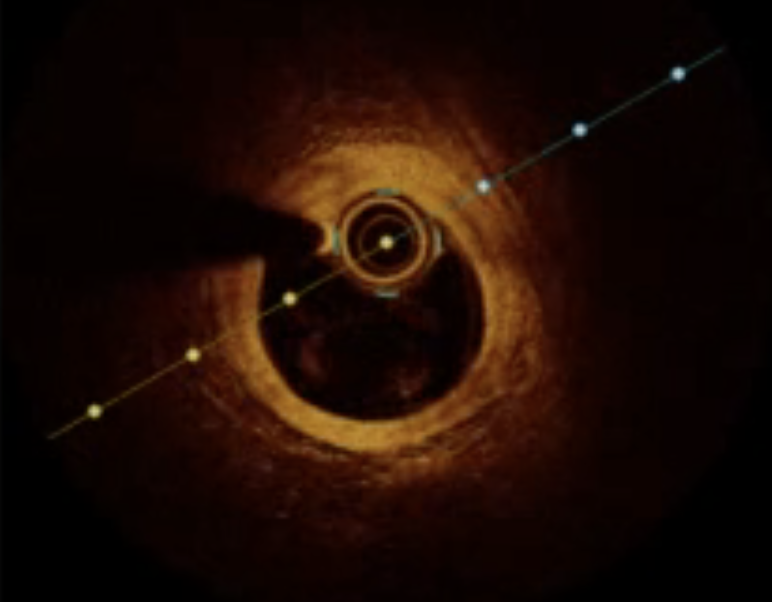
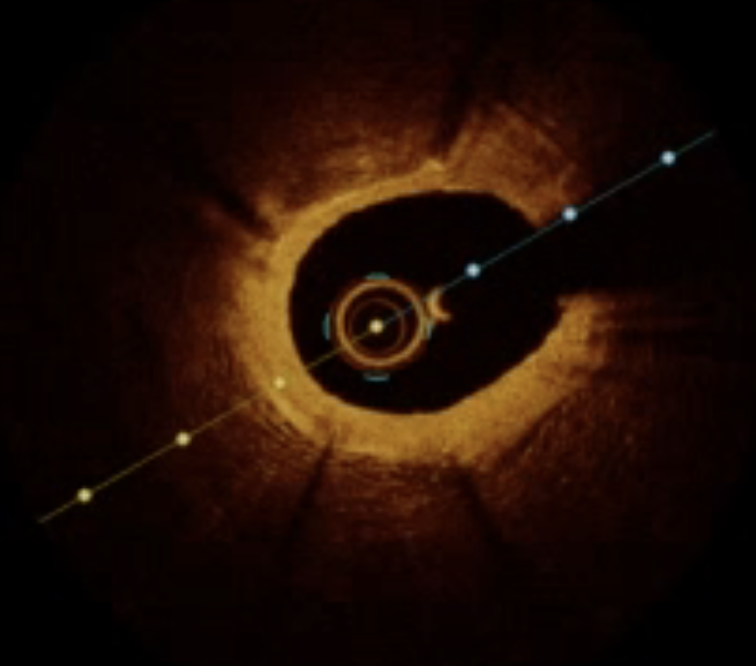
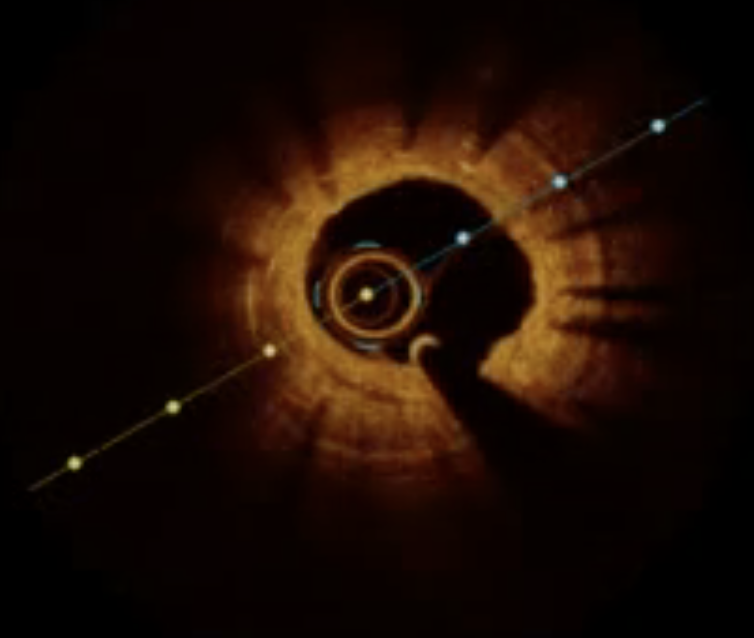
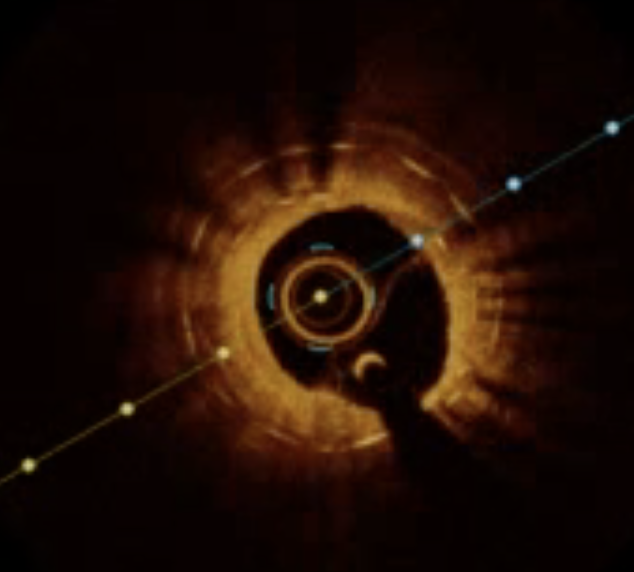
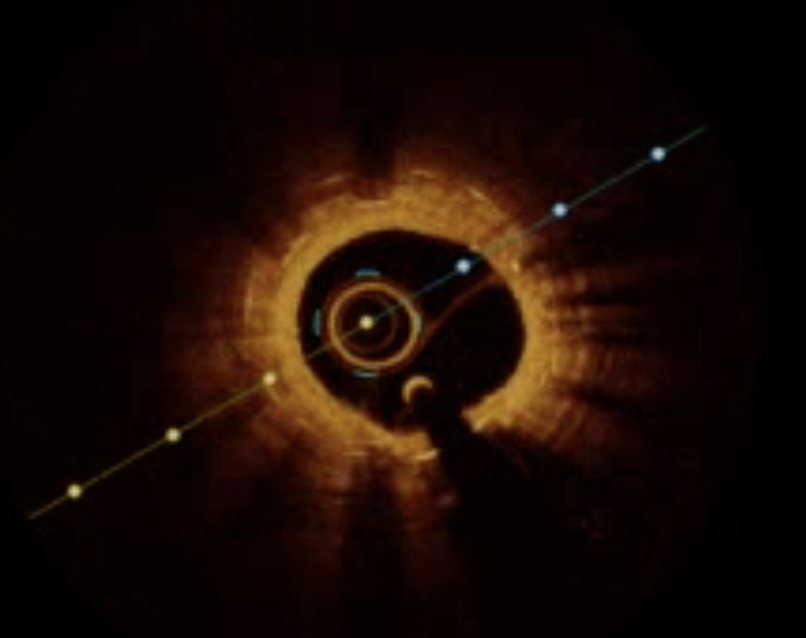
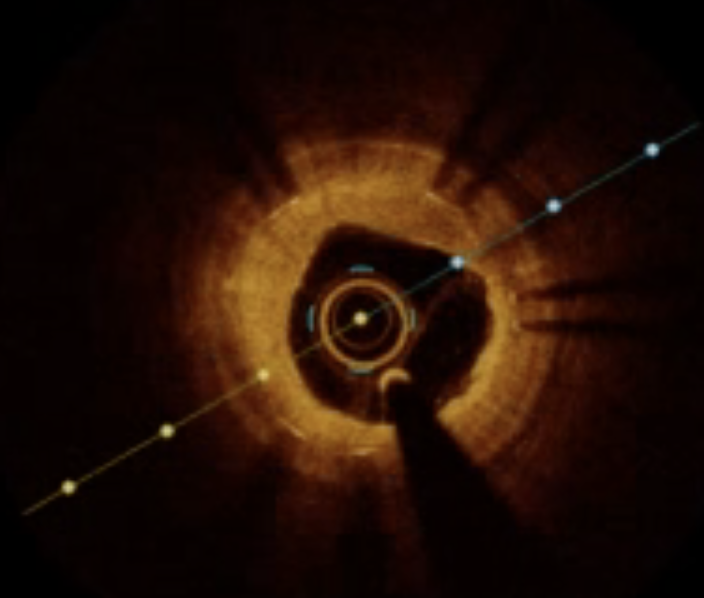
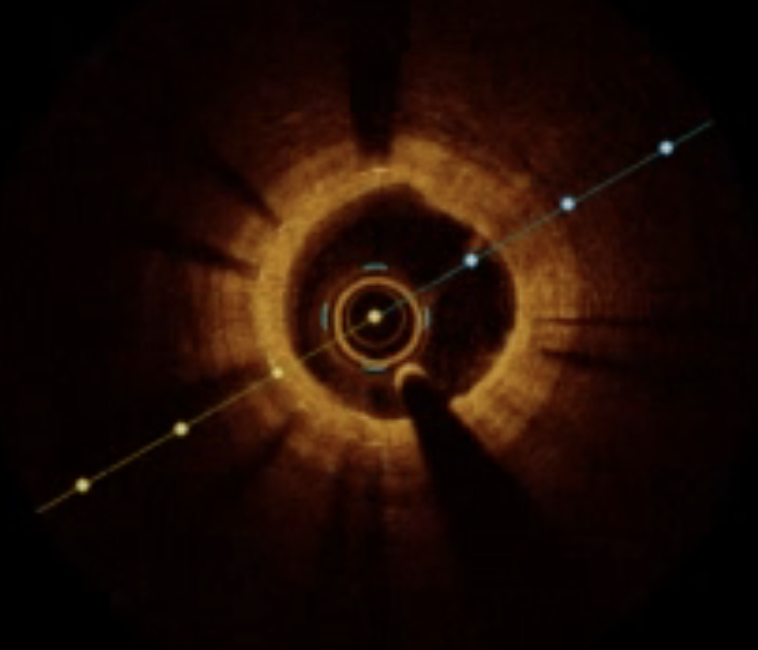
Send the ebu3.75 guiding tube to the left coronary, and measure the lad FFR 0.78 with Abbott pressure wire x 0.014-175cm pressure guide wire, and send it to dragonfly Optis imaging catheter 2.7f-135cm catheter for lad OCT examination, which indicates diffuse fibrous tissue hyperplasia and neo-plaques in m-dLAD stent. And the two-layer stent does not fit completely. dlad MSA is 1.08mm2, mLAD MSA 2.37mm2; The lesions were fully pre dilated with trek 2.0-20mm and NC trek 2.5-15mm & 3.0-15mm. After DCB 2.5-30mm & 3.0-26mm treatment (all 10ATM), OCT was rechecked, dLAD MSA 2.7mm2 and mLAD MSA 4.24mm2; Retest FFR 0.89.
DCB1.mp4
DCB2.mp4
Fianl2.mp4
Final.mp4
Case Summary
The patient was followed up for more than one year without any symptoms. The causes of LAD ISR in this case are very complex, including fibrous tissue hyperplasia, new atherosclerotic plaque and mechanical factors. It is very successful to guide DCB treatment with OCT and FFR.