
Lots of interesting abstracts and cases were submitted for TCTAP 2022. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-088
The Road Less Traveled: Rotational Atherectomy of the Left Anterior Descending and Left Circumflex Arteries in a Heavily Calcified and Critical True Left Main Bifurcation on the Background of Non ST Elevation Myocardial Infarction With Cardiogenic Shock Using Double Guiding Catheter
By Kristy Garganera, Bryan Rene Toledano, Francis Charles Fernandez, Michelangelo L. Sabas
Presenter
Kristy Brillantes Garganera
Authors
Kristy Garganera1, Bryan Rene Toledano1, Francis Charles Fernandez1, Michelangelo L. Sabas1
Affiliation
The Medical City, Philippines1,
View Study Report
TCTAP C-088
CORONARY - Complex and Higher Risk Procedures for Indicated Patients (CHIP)
The Road Less Traveled: Rotational Atherectomy of the Left Anterior Descending and Left Circumflex Arteries in a Heavily Calcified and Critical True Left Main Bifurcation on the Background of Non ST Elevation Myocardial Infarction With Cardiogenic Shock Using Double Guiding Catheter
Kristy Garganera1, Bryan Rene Toledano1, Francis Charles Fernandez1, Michelangelo L. Sabas1
The Medical City, Philippines1,
Clinical Information
Patient initials or Identifier Number
F.G.
Relevant Clinical History and Physical Exam
83 yo female hypertensive, poorly controlled diabetic. 3 hours prior complained of chest pain and shortness of breath hence brought to ER, after which she had sudden cardiac arrest. ACLS done and ROSC achieved after 8 minutes. On PE pupils were isocoric & sluggishly reactive, GCS 10, fine bibasal crackles, no appreciable murmurs, apex beat at the 5th ICS, anterior axillary line. BP 90-100/60 on norepinephrine 0.3mcg/kg/min & dobutamine 5mkd.
Relevant Test Results Prior to Catheterization
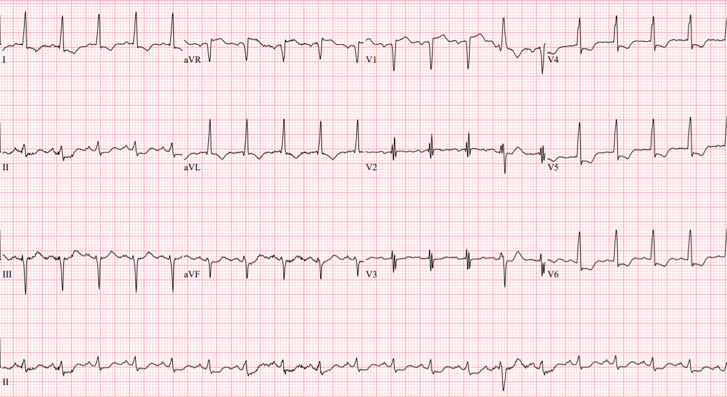
ECG 12 leads: ST segment elevation in leads aVR and V1 with diffuse ST segment depression in other leadsChest Xray: Congestion; atherosclerotic aortaHS Troponin I: 1053 pg/mL
Relevant Catheterization Findings
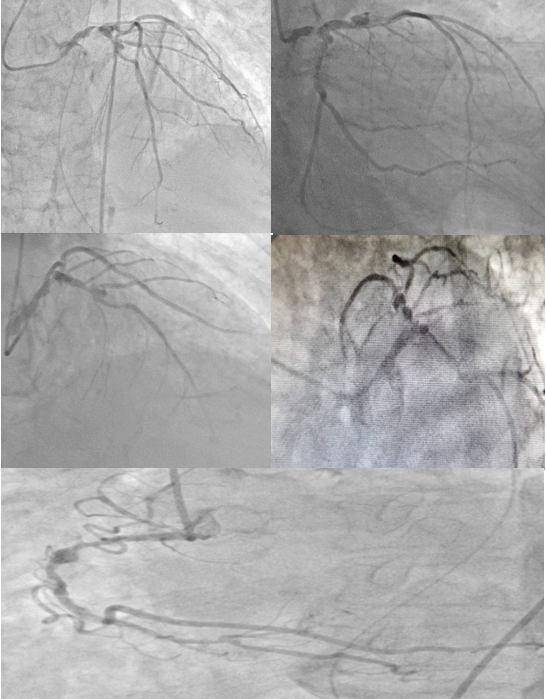
LM 4.5mm with 95% distal stenosis with heavy calcification at the distal LMCA extending to ostio-proximal LAD and LCx. LAD 4mm type II vessel with TIMI 2 flow. It has a diffuse long segment proximal stenosis of 70%. Ramus intermedius fair sized diffusely diseased vessel. LCx 4mm vessel with diffusely diseased proximal segment of 80%. RCA 3.5mm dominant diffusely diseased vessel with worst stenosis of 70%. It has a pre-stenotic mid segment dilatation.
 F.G. (cranial).avi
F.G. (cranial).avi
F.G. (LAO CAUD).avi
Interventional Management
Procedural Step
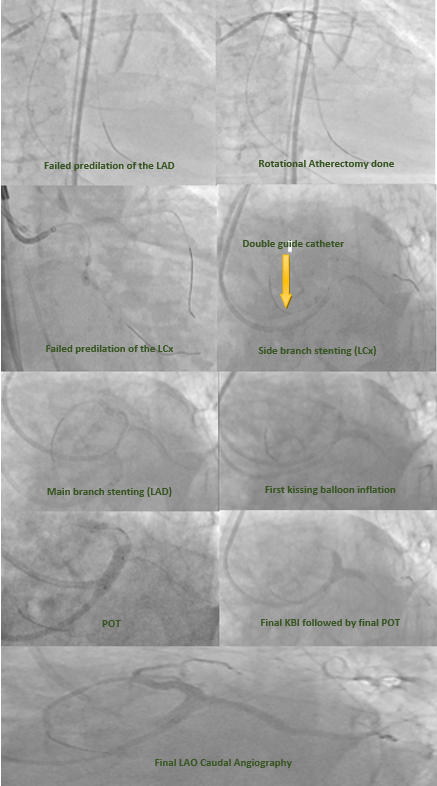
Support: IABP left femoral arteryAccess 1: right femoral arteryGuide & guidewire: 6F, Asahi Sion to LADPredilation of proximal LAD: 2.5x15mm balloon exchanged to 2.5x8mm due to undilatable focal segment1st rotational atherectomy using 1.25mm burr with floppy wireAccess 2: right radial arteryGuide & guidewire: 6F, Asahi Sion Blue to terminal OMPredilation of LCx: 2.0x20mm balloon upsized to 2.5x6mm due to undilatable focal segment
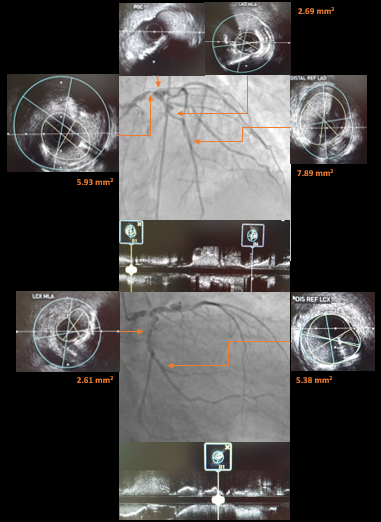
2nd rotational atherectomy using 1.25mm burr with extra support wireIVUS run: mixed to circumferential calcified plaques from mid LAD to distal LM and mid LCx to distal LM,LAD MLA 2.76mm2,LCx MLA1.90mm2,LM MLA 2.76mm2Stent1: 2.5x28mm DES at proximal terminal OM to midLCxStent2: 2.5x24mm DES at mid to proximal LAD
SB stent: 3.0x24mm DES at proximal LCx to distal LMBalloon crush: 3.5x15mm balloon at the LAD then nondistal SB rewiring1st KBI and POT: sequential balloon inflation of a 3.5x15mmballoon positioned at the LCx to LM and LAD to LM followed by KBI and POTMV stent: 4.0x24mm DES at proximal LAD to LMPOT: 4.0x24 stent balloon at proximal LM to level of carina then nondistal SB rewiringFKBI: sequential balloon inflation of a 3.5x15mm balloon positioned at the LCx to LM and LAD to LMFinal POT: 4.5x12mm balloon at LM up to carina levelIVUS run: good stent apposition LAD MSA 12.59mm2,LCx MSA6.79mm2,LM MSA 12.59mm2, no stent edge dissection within 3mmPost PCI angiography: TIMI 3 flow, no perforation
F.G. (PINGPONG CATHETER).avi
2nd rotational atherectomy using 1.25mm burr with extra support wireIVUS run: mixed to circumferential calcified plaques from mid LAD to distal LM and mid LCx to distal LM,LAD MLA 2.76mm2,LCx MLA1.90mm2,LM MLA 2.76mm2Stent1: 2.5x28mm DES at proximal terminal OM to midLCxStent2: 2.5x24mm DES at mid to proximal LAD
SB stent: 3.0x24mm DES at proximal LCx to distal LMBalloon crush: 3.5x15mm balloon at the LAD then nondistal SB rewiring1st KBI and POT: sequential balloon inflation of a 3.5x15mmballoon positioned at the LCx to LM and LAD to LM followed by KBI and POTMV stent: 4.0x24mm DES at proximal LAD to LMPOT: 4.0x24 stent balloon at proximal LM to level of carina then nondistal SB rewiringFKBI: sequential balloon inflation of a 3.5x15mm balloon positioned at the LCx to LM and LAD to LMFinal POT: 4.5x12mm balloon at LM up to carina levelIVUS run: good stent apposition LAD MSA 12.59mm2,LCx MSA6.79mm2,LM MSA 12.59mm2, no stent edge dissection within 3mmPost PCI angiography: TIMI 3 flow, no perforation
Case Summary
A heavily calcified left main bifurcation and undilatable left anterior descending artery and left circumflex artery presenting as NSTEACS with cardiogenic shock is a nightmare. A rotational atherectomy of both main vessels can be done to prepare the lesion and improve the hemodynamics. Employing a DK crush technique using double guide catheter lessens the chance of wire entanglement and may improve efficiency.