
Lots of interesting abstracts and cases were submitted for TCTAP 2022. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-046
Recurrent NSTEMI in Post CABG Patient : What's Next?
By Cut Aryfa Andra, Faisal Habib, Anggia Chairuddin Lubis, Muhammad Yolandi Sumadio
Presenter
Cut Aryfa Andra
Authors
Cut Aryfa Andra1, Faisal Habib2, Anggia Chairuddin Lubis3, Muhammad Yolandi Sumadio3
Affiliation
Department of Cardiology and Vascular Medicine, Faculty of Medicine, Universitas Sumatera Utara, Indonesia1, General Hospital H. Adam Malik, Indonesia2, University of Sumatera Utara, Indonesia3,
View Study Report
TCTAP C-046
CORONARY - Bifurcation/Left Main Diseases and Intervention
Recurrent NSTEMI in Post CABG Patient : What's Next?
Cut Aryfa Andra1, Faisal Habib2, Anggia Chairuddin Lubis3, Muhammad Yolandi Sumadio3
Department of Cardiology and Vascular Medicine, Faculty of Medicine, Universitas Sumatera Utara, Indonesia1, General Hospital H. Adam Malik, Indonesia2, University of Sumatera Utara, Indonesia3,
Clinical Information
Patient initials or Identifier Number
Mr NS
Relevant Clinical History and Physical Exam
50 y.o Indonesian man, with risk factors for CAD were smoker, diabetes mellitus type 2, hypertension and obese. He came to ER with recurrent chest pain and diagnosed as recurrent Acute Coronary Syndrome for 3 times in the last one year. He had CABG with 3 grafts in 2018, LIMA was grafted to LAD, SVG to LCX, and SVG to RCA. Underwent stenting LCX in 2016. Vital signs were normal. Physical exemination was normal
Relevant Test Results Prior to Catheterization
ECG showed anterior ischemia. Echocardiography showed good LV systolic with EF 58%. LV diastolic dysfunction grade I with normal LAP. Wall motion was global normokinetic. Good RV contractility with TAPSE 19 mm.Chest X-ray was mild cardiomegaly. Troponin T level was markedly raised, random blood glucose and HbA1C were increased. Other blood test were normal. He was diagnosed as high risk Non-ST Elevation Myocardial Ischemia (NSTEMI)
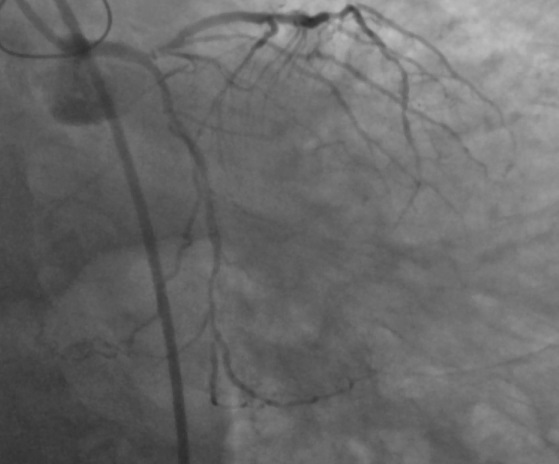
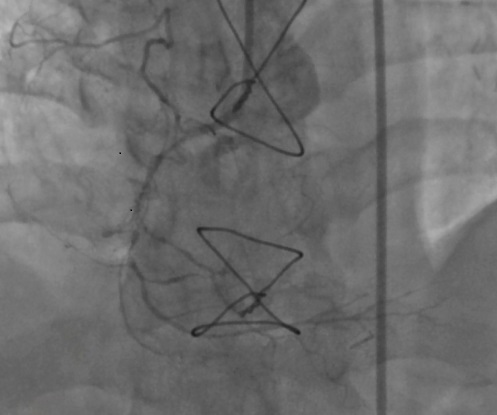
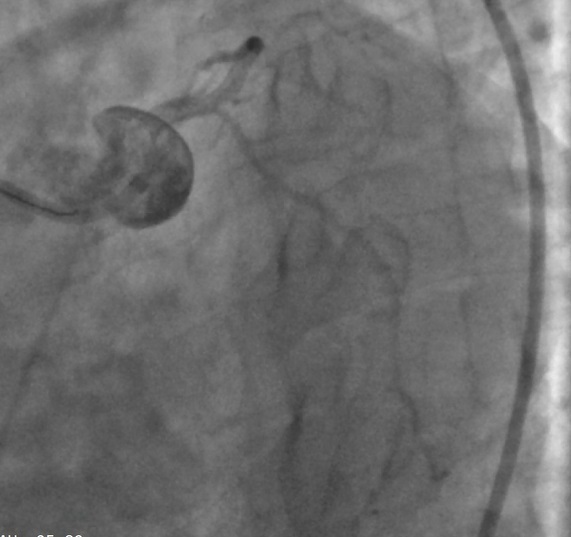
Relevant Catheterization Findings
He had bifurcation lesion Medina 1, 1, 0 at mid-distal shaft LM stenosis 50%. LAD subtotal occlusion at osteal, stenosis 80% at mid and musle bridging at mid LAD. LCX stenosis 30-40% before stent, good previous stent. RCA stenosis 80% at proximal, CTO before RV branch. Graft SVG-RCA couldn't visualize. Graft SVG-LCX was good. Graft LIMA-LAD was small caliber, diffuse stenosis, failed. The conclusion of coronary angiography was CAD 3VD with Graft failure.
 Caudal.wmv
Caudal.wmv
LIMA-LAD.wmv
RCA.wmv
SVG-LCX.wmv

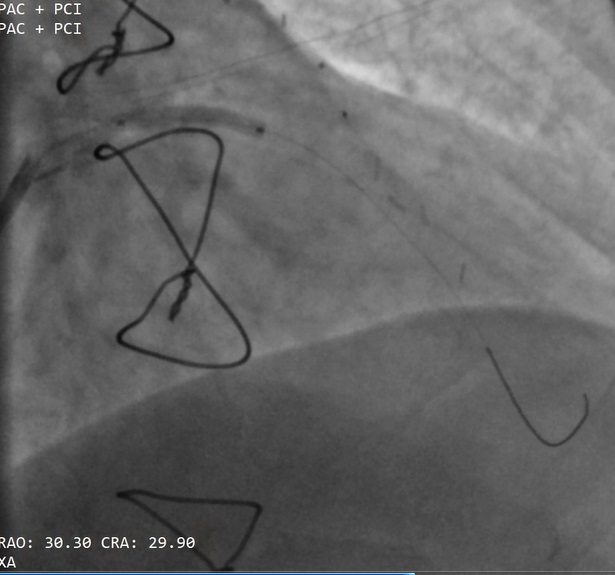
Interventional Management
Procedural Step
We perfomed provisional stenting LM bifurcation PCI. Left coronary artery was engaged with 7F EBU via right femoral artery. Runthrough wired into LAD. Predilatation done at proximal LAD with Sprinter Legend Balloon 1,5 x 15, inflated until 18 atm, 10 sec, continued with Scoroflex Balloon 2,5 x 15 mm LM to LAD proximal inflated until 10 atm, 8 sec.Proximal to mid LAD was stented with drug eluting stent (DES) Resolute Integrity 2,75 x 18 mm, 8atm, 6 sec, followed by stented LM osteal to LAD proximal with DES Resolute Integrity 3,0 x 26 mm, inflated 9 atm,6 sec (overlapped). Proximal optimization technique was done at LM with NC Sprinter Balloon 3,5 x 12 mm, 13 atm, 8 sec.
Balloon 1,5x15.wmv
Balloon 2,5x15.wmv
Stent 2,75x18.wmv
Stent 3x26.wmv
POT LAO CRA.wmv
POT Spider.wmv
POT.wmv
RAO CAU Post POT.wmv
RAO CRA Post POT.wmv
Spider Post POT.wmv

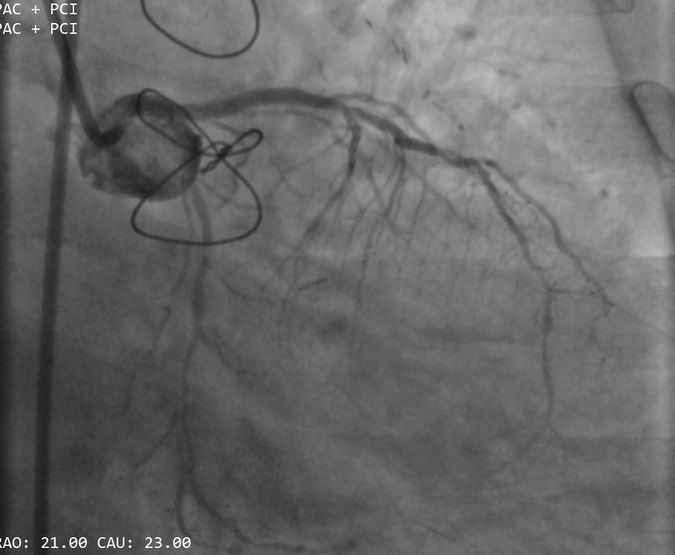
Case Summary
Provisional stenting of the LM to LAD with Medina classification 1, 1, 0 was done. Patient was discharged well after 2 days. Follow up 6 months after PCI remained well and asymptomatic. Redo CABG is associated with higher mortality and higher of perioperative myocardial infarction. PCI is preferred method of treating patients post CABG with graft failure. Provisional stenting is simpler bifurcation technique and should be the technique of choice in bifurcation strategy. The successful rate will be higher if the procedure is well planned.