
Lots of interesting abstracts and cases were submitted for TCTAP 2022. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-024
The Road Less Travelled
By Kogulakrishnan Kaniappan, Balachandran Kandasamy, Beni Isman Rusani, Afrah Yousif Haroon, David Yong
Presenter
Kogulakrishnan Kaniappan
Authors
Kogulakrishnan Kaniappan1, Balachandran Kandasamy2, Beni Isman Rusani1, Afrah Yousif Haroon1, David Yong1
Affiliation
National Heart Institute, Malaysia1, Subang Jaya Medical Centre, Malaysia2,
View Study Report
TCTAP C-024
CORONARY - Adjunctive Procedures (Thrombectomy, Atherectomy, Special Balloons)
The Road Less Travelled
Kogulakrishnan Kaniappan1, Balachandran Kandasamy2, Beni Isman Rusani1, Afrah Yousif Haroon1, David Yong1
National Heart Institute, Malaysia1, Subang Jaya Medical Centre, Malaysia2,
Clinical Information
Patient initials or Identifier Number
BGM
Relevant Clinical History and Physical Exam
62 years old lady , with recent admission for Unstable Angina, presented with chest pain for 1 week.
Onexamination :
Onexamination :
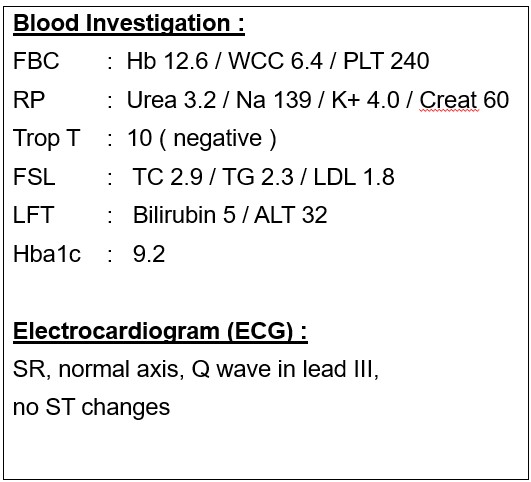
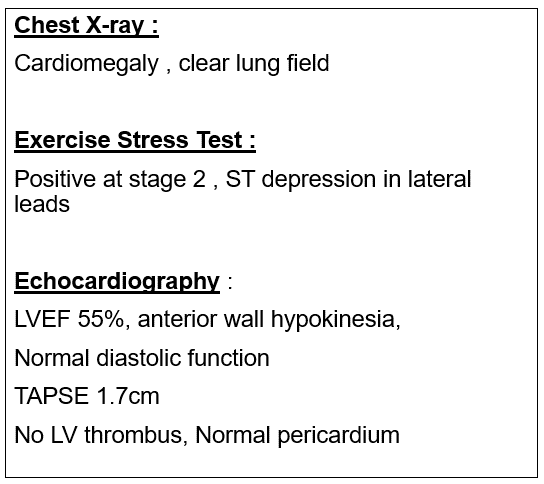
Relevant Test Results Prior to Catheterization
BloodInvestigation :
Relevant Catheterization Findings
LMS : mild ISR Left Main Stem stent
 Left coronary sytem angiogram.avi
Left coronary sytem angiogram.avi
Righ coronary system angiogram.avi
NC Trek 3.0x12mm failed to expand fully.avi
Interventional Management
Procedural Step
Staged PCI to LM/LAD +/- LCX
IVL shockwave balloon used in LAD.avi
Same IVL shockwave balloon used to predilate LCX.avi
Final results after final POT balloon.avi
Case Summary
- Novel usage of Intravascular Lithotripsy in Severe In-stent Restenosis (ISR) with the background of coronary artery calcification (CAC), especially in calcified nodule is a viable and safe option, compared to other atherectomy devices.
- Deployment of same IVL balloon catheter in 2 different vessels is feasible and effective, as demonstrated in our novel case using this approach.
- Further prospective trials and clinical evidences required to review and expand the indication of IVL in such selected cases.