
Lots of interesting abstracts and cases were submitted for TCTAP 2022. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-017
Where Is the Culprit? - A Triple Vessels Disease Acute Coronary Syndrome With Tortuous Aorta
By Chun Yu Fung
Presenter
Chun Yu Fung
Authors
Chun Yu Fung1
Affiliation
Tuen Mun Hospital, Hong Kong, China1,
View Study Report
TCTAP C-017
CORONARY - Acute Coronary Syndromes (STEMI, NSTE-ACS)
Where Is the Culprit? - A Triple Vessels Disease Acute Coronary Syndrome With Tortuous Aorta
Chun Yu Fung1
Tuen Mun Hospital, Hong Kong, China1,
Clinical Information
Patient initials or Identifier Number
Mr. L
Relevant Clinical History and Physical Exam
81 year old gentleman who is a chronic smoker and drinker, with past medical history of diabetes and hypertension.
Presented to us for one day history of chest pain with radiation to shoulder. No radiation to the back
Physical exam is unremarkable and show no sign of heart failure.
Relevant Test Results Prior to Catheterization
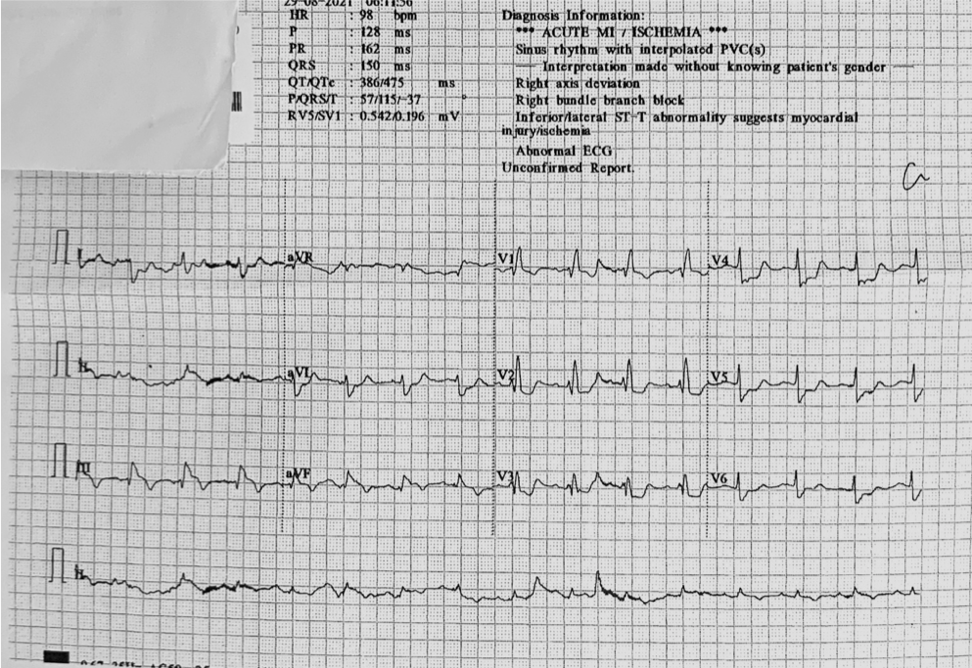
ECG show ST-elevation over inferior leads ( III > II), ST- depression over V2-6. underlying old RBBB
ddx: 1. double culprit with RCA and LCx 2. dominant RCA STEMI
Trop I 1300 > 30453> 26316
Echocardiogram
´Normal chambers size
´LV ejection fraction 42% by Simpson’s
´HK over inferior and inferoseptal wall
´No pericardial effusion
Relevant Catheterization Findings
Weak radial pulse, R femoral artery approach used
Tortuous R common femoral artery.
Fail to advance 7Fr 45cm long sheath
Exchange to Amplatzer supper stiff guidewire with 7Fr 23cm sheath
LM: normal
LAD: calcified vessels, pLAD 90% stenosis, mLAD critical lesion
LCx: mLCx critical lesion, distal diffuse disease
RCA: dominant RCA, pRCA 70% stenosis, mRCA 50% stenosis, dRCA 90% with ulcerative plaque and haziness . PL 90% stenosis
Indirect angiogram to L CFA with 6Fr pigtail catheter show less tortuous L CFA
Interventional Management
Procedural Step
Tortuous R common femoral artery. Cordis guidewire cannot negotiate through
Exchange to Terumo guidewire
Try to advance 7Fr 45cm long sheath but fail.
Exchange to Amplatzer supper stiff guidewire with 7Fr 23cm sheathDiscussed with family x CABG vs PCI. Opted for the latter
Plan for multi-stage PCI.
PCI to RCA lesion first because it is the culprit lesion and complex left system lesion
Runthrough NS passed to PL
mRCA and dRCA lesion predilated with Raiden 2.5/15
IVUS done for lesion characterisation and landing zone planning
Limited distal landing zone, decide to stent from proximal to distal lesion
Fail to pass stent to PL, further prepare mRCA lesion with NC trek 3.5/15
pRCA-mPL stented with overlapping Xience Sierra 3.5/38, Xience Xpedition3.5/48 and Xience Sierra 4.0/38
Stent post dilated with NC Trek 3.5/15 and 4.0/15
Case Summary
Successful IVUS guided PTCA/S done to pRCA to mPL.ECG in this case show possible double culprit with ST elevation in lead III higher than lead II and also ST depression over lateral leads.Long sheath is commonly used for tortuous aorta, if fail we can try super stiff wire to straighten the vessel,