
Lots of interesting abstracts and cases were submitted for TCTAP 2022. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-157
Coronary Physiology Assessment in a Patient With Triple Vessel Disease and Chronic Total Occlusion
By Koon Wee Koay, Goh Chong Aik, Shahul Hamid K A Ahmadsah, Poi Keong Kong, Muhamad Ali SK Abdul Kader
Presenter
Koon Wee Koay
Authors
Koon Wee Koay1, Goh Chong Aik2, Shahul Hamid K A Ahmadsah3, Poi Keong Kong1, Muhamad Ali SK Abdul Kader4
Affiliation
Penang General Hospital, Malaysia1, Kpj Penang Specialist Hospital, Malaysia2, Hospital Pulau Pinang, Malaysia3, Sultan Idris Shah Serdang Hospital, Malaysia4,
View Study Report
TCTAP C-157
IMAGING AND PHYSIOLOGIC LESION ASSESSMENT - Physiologic Lesion Assessment
Coronary Physiology Assessment in a Patient With Triple Vessel Disease and Chronic Total Occlusion
Koon Wee Koay1, Goh Chong Aik2, Shahul Hamid K A Ahmadsah3, Poi Keong Kong1, Muhamad Ali SK Abdul Kader4
Penang General Hospital, Malaysia1, Kpj Penang Specialist Hospital, Malaysia2, Hospital Pulau Pinang, Malaysia3, Sultan Idris Shah Serdang Hospital, Malaysia4,
Clinical Information
Patient initials or Identifier Number
Madam LCY
Relevant Clinical History and Physical Exam
Madam LCY is a 70 years old lady who has underlying hypertension, diabetes mellitus and end-stage renal disease on regular haemodialysis. She presented with frequent episodes of chest pain during haemodialysis and intradialytic hypotension for 1 month.
Relevant Test Results Prior to Catheterization
ECG showed sinus rhythm and Q wave at lead III. Echocardiography showed a left ventricular ejection fraction of 55 % and hypokinesia at inferolateral, inferoseptal and inferior wall.
Relevant Catheterization Findings
Coronary angiography showed 70 % stenosis at mid-left anterior descending (LAD) artery, 70 % stenosis at mid-left circumflex (LCX) artery and a chronic total occlusion (CTO) at proximal right coronary artery (RCA) with retrograde flow from LAD. The calculated SYNTAX I score was 18.0 and SYNTAX II score was 49.7.
 ap cranial.wmv
ap cranial.wmv
lao caudal.wmv
lao.wmv
Interventional Management
Procedural Step
Bilateral femoral artery puncture was done with 6Fr femoral sheath. Coronary guide catheter 6Fr XB 3.5 was used for left coronary artery and 6F AL 1.0 was used for RCA. Coronary physiology was done to LAD and LCX prior to coronary intervention. Intracoronary adenosine 200mcg bolus was used for hyperaemia. Fractional flow reserve (FFR) value of LAD was positive with 0.76 and FFR value of LCX was negative with 0.9. FFR of RCA was not done as it was a CTO at proximal RCA.
cross bilateral inj lao.wmv
last shot no wire lao.wmv
Case Summary
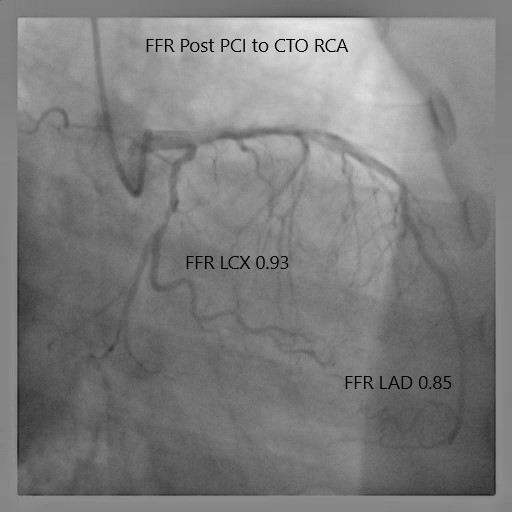
From visual angiography assessment, this patient has triple vessel disease with a CTO at RCA which received collateral flow from a diseased LAD. Pre-PCI FFR assessment showed negative ischaemia at LCX and positive ischaemia at LAD. After revascularization of CTO RCA, the LAD's FFR has changed from positive to negative. This is because the LAD perfusion territory was reduced as it no longer needed to provide collateral flow to RCA. The use of FFR has reduced the number of stents required in this patient and has changed a CABG strategy to a single vessel PCI. This case highlights the importance of coronary physiology guided PCI which will provide a better outcome for the patient.