
Lots of interesting abstracts and cases were submitted for TCTAP 2022. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-052
A Case of Successful Rotational Atherectomy in a Heavily Calcified, Uncrossable Chronic Total Occulsion Lesion
By Jin Jung, Sung-Ho Her
Presenter
Jin Jung
Authors
Jin Jung1, Sung-Ho Her1
Affiliation
The Catholic University of Korea, St. Vincent's Hospital, Korea (Republic of)1,
View Study Report
TCTAP C-052
CORONARY - Chronic Total Occlusion
A Case of Successful Rotational Atherectomy in a Heavily Calcified, Uncrossable Chronic Total Occulsion Lesion
Jin Jung1, Sung-Ho Her1
The Catholic University of Korea, St. Vincent's Hospital, Korea (Republic of)1,
Clinical Information
Patient initials or Identifier Number
KYG
Relevant Clinical History and Physical Exam
A 56-year-old male patient who had a history of NSTEMI with underlying hypertension and diabetic chronic kidney disease presented to a district hospital with worsening dyspnea.

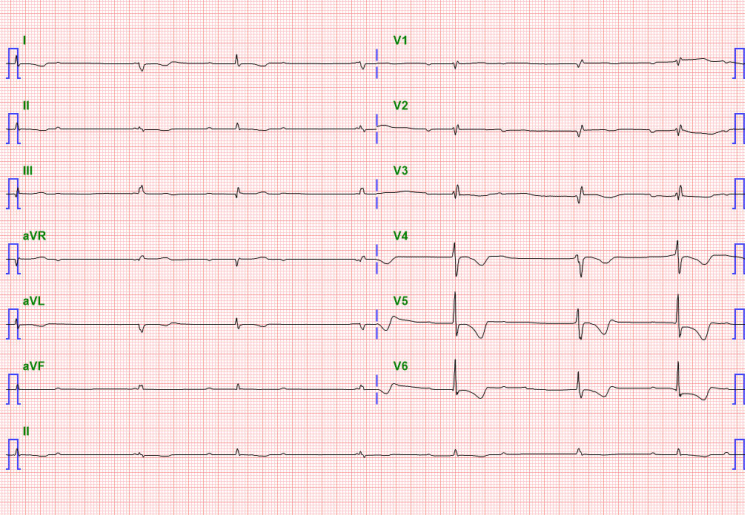
Relevant Test Results Prior to Catheterization
The echocardiogram showed LV systolic dysfunction (EF 33.7%) with akinesis at basal to mid inferior, inferolateral LV wall motion and decreased RV function (TAPSE 15.6mm)
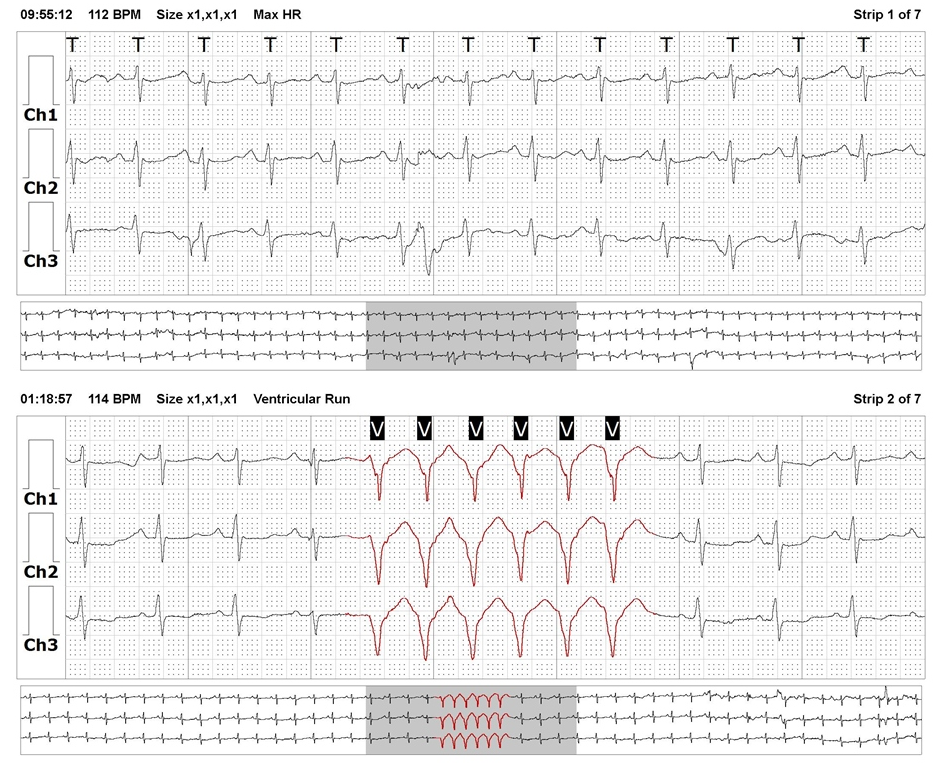
PCI was attempted to the RCA CTO lesion, but the patient seizure with complete AV block during the procedure. After guiding catheter pull back to aorta, vital sign was recovered and procedure was stopped.
24 hours holter showed NSVT and intermittent high degree AV block. So ICD implantation was performed before PCI retry.
PCI was attempted to the RCA CTO lesion, but the patient seizure with complete AV block during the procedure. After guiding catheter pull back to aorta, vital sign was recovered and procedure was stopped.
24 hours holter showed NSVT and intermittent high degree AV block. So ICD implantation was performed before PCI retry.
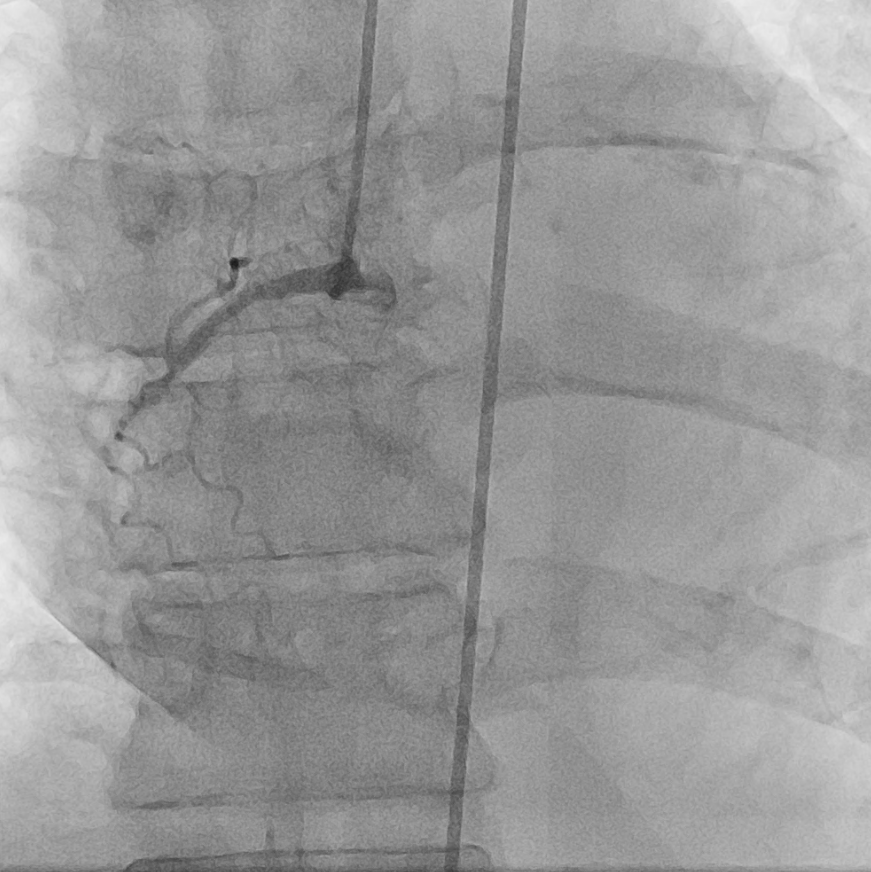
Relevant Catheterization Findings
Coronary Angiography LM : minimal lesionLAD : pdLAD 30 % stenosis. diffuse, concentric, smooth, TIMI 3LCx : LCx Os 95 % stenosis. discrete, eccentric, smooth, TIMI 3RCA : mRCA 100 % stenosis. CTO lesion, TIMI 0, collateral vessel Grade 1 from LAD septal br
 LM-angio.avi
LM-angio.avi
RCA-angio.avi
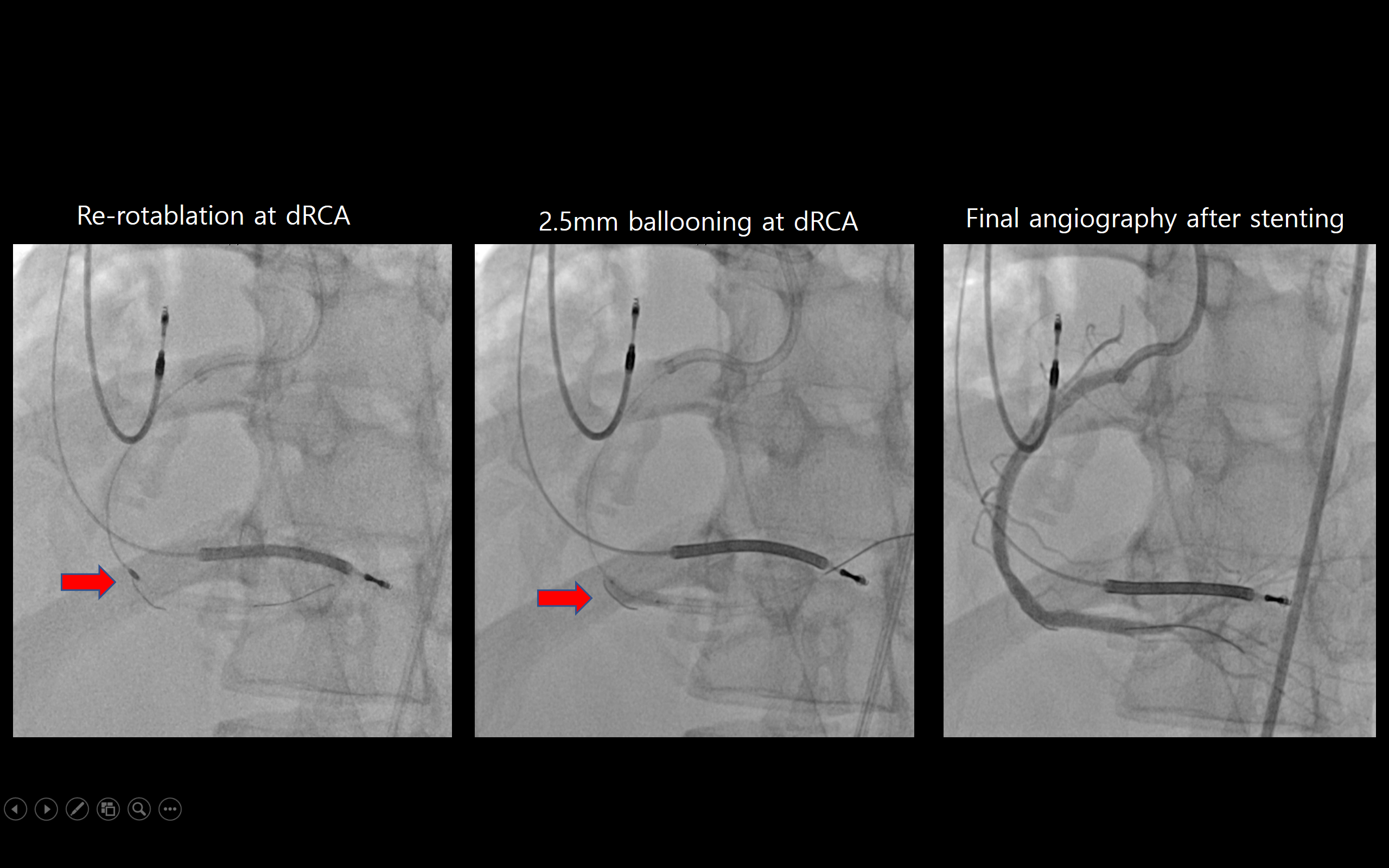
Interventional Management
Procedural Step
PCI was done to mdRCA CTO lesion with 100% ISR at dRCA
mRCA.avi

Case Summary
Rotational atherectomy is useful in heavy calcified CTO lesion that was not passed by device.