
Lots of interesting abstracts and cases were submitted for TCTAP 2022. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-012
Stormy Primary Percutaneous Coronary Intervention During COVID-19 Pandemic
By Wei Juan Lim, Hoong Sheng Loh, Ting Yuen Beh, Balachandran Kandasamy
Presenter
Wei Juan Lim
Authors
Wei Juan Lim1, Hoong Sheng Loh1, Ting Yuen Beh1, Balachandran Kandasamy2
Affiliation
National Heart Institute, Malaysia1, Subang Jaya Medical Centre, Malaysia2,
View Study Report
TCTAP C-012
CORONARY - Acute Coronary Syndromes (STEMI, NSTE-ACS)
Stormy Primary Percutaneous Coronary Intervention During COVID-19 Pandemic
Wei Juan Lim1, Hoong Sheng Loh1, Ting Yuen Beh1, Balachandran Kandasamy2
National Heart Institute, Malaysia1, Subang Jaya Medical Centre, Malaysia2,
Clinical Information
Patient initials or Identifier Number
TPS HK
Relevant Clinical History and Physical Exam
85-year-old patient with underlying hypertension, dyslipidemia presented with chest pain for 2 days duration, radiating to left shoulder with shortness of breath to our emergency department. Blood pressure was 130/80 mmHg with heart rate of 80bpm. There was no murmur and lungs showed bibasal crepitation.
Relevant Test Results Prior to Catheterization
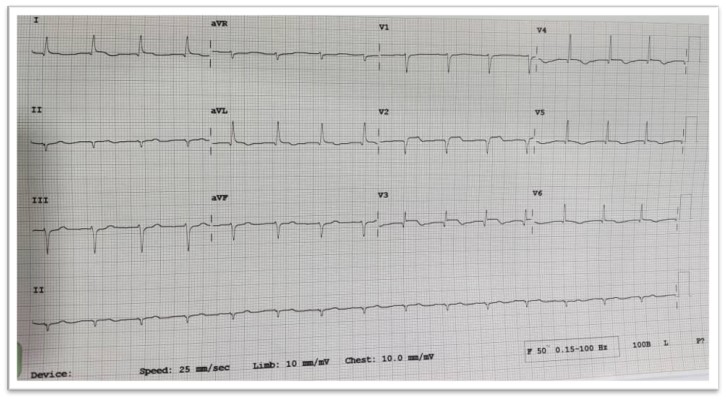
Electrocardiogram at emergency department showed ST elevation at anterolateral leads with ST depression at inferior leads. Patient was diagnosed with acute anterolateral ST elevation myocardial infarction (STEMI) and catheterization lab was activated for primary percutaneous coronary intervention (PCI).
Relevant Catheterization Findings
Primary PCI team has been alerted and everyone wore full personal protection equipment as universal precaution prior to starting procedure. Vessel assessed via right femoral approach, using JR 3.5 6Fr showing mild disease at mid right coronary artery.
Left system was engaged with EBU 3.0 6Fr which showed mild disease mid to distal left main stem, mild disease mid left circumflex artery and severe stenosis proximal left anterior descending artery and ostial diagonal 1.
 RCA RAO.mpg
RCA RAO.mpg
RAO CRA.mpg
CAU.mpg
Left system was engaged with EBU 3.0 6Fr which showed mild disease mid to distal left main stem, mild disease mid left circumflex artery and severe stenosis proximal left anterior descending artery and ostial diagonal 1.
Interventional Management
Procedural Step
EBU 3.0 6Fr was used to engage left system. After diagnostic shots were taken, noted patient became bradycardia and subsequently asystole. Cardiopulmonary resuscitation (CPR) was started according to advanced cardiac life support. Primary PCI continued during CPR with wiring down LAD with Sion Blue wire. There was difficulty in wiring through severe stenosis at LAD and hence balloon support technique was used.
After crossing stenosis at proximal LAD, an attempt to pass Thrombuster but failed. Stenotic lesion at proximal LAD was balloon using Sapphire 2.5x15 mm and then 3.0x15 mm. Post-balloon dilatation, Thrombuster able to pass through but only noted minimal thrombus after suction.
Runthrough floppy was wired to diagonal 1 and subsequently stented with Xience Sierra 3.0x30 mm. Stent was post dilated with Sapphire non-compliance balloon 3.5x15 mm.
During PCI, patient was intubated by anesthesiology team and CPR continued. Return of spontaneous circulation (ROSC) attained post PCI and patient was sent to coronary care unit (CCU) for close monitoring.
after 2 ballon.mpg
RTF Sierra.mpg
Final CRA.mpg
After crossing stenosis at proximal LAD, an attempt to pass Thrombuster but failed. Stenotic lesion at proximal LAD was balloon using Sapphire 2.5x15 mm and then 3.0x15 mm. Post-balloon dilatation, Thrombuster able to pass through but only noted minimal thrombus after suction.
Runthrough floppy was wired to diagonal 1 and subsequently stented with Xience Sierra 3.0x30 mm. Stent was post dilated with Sapphire non-compliance balloon 3.5x15 mm.
During PCI, patient was intubated by anesthesiology team and CPR continued. Return of spontaneous circulation (ROSC) attained post PCI and patient was sent to coronary care unit (CCU) for close monitoring.
Case Summary
Primary PCI during COVID-19 pandemic is challenging with full PPE. PCI during CPR is technically challenging as well but it is possible with experienced operator. We should not give up easily during procedure but to try our best in giving the best care to our patients during COVID-19 pandemic.