
Lots of interesting abstracts and cases were submitted for TCTAP 2022. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-123
Embolic Shower to Coronary and Cerebral Arteries From a Cardiac Myxoma
By Ghiath Baroudy, Fahmi Othman, Ahmed Mahfouz, Sherif Helmy, Ihsan Rafie, Abdulaziz Abdulla AL Khulaifi
Presenter
Ghiath Sadek Baroudy
Authors
Ghiath Baroudy1, Fahmi Othman2, Ahmed Mahfouz2, Sherif Helmy3, Ihsan Rafie4, Abdulaziz Abdulla AL Khulaifi2
Affiliation
Hamad Medical Corporation Heart Hospital, Qatar1, HMC Heart Hospital, Qatar2, Heart Hospital Hamad Medical Corporation, Qatar3, Hamad Medical Corporation (HMC), Doha, Qatar4,
View Study Report
TCTAP C-123
CORONARY - Hemodynamic Support and Cardiogenic Shock
Embolic Shower to Coronary and Cerebral Arteries From a Cardiac Myxoma
Ghiath Baroudy1, Fahmi Othman2, Ahmed Mahfouz2, Sherif Helmy3, Ihsan Rafie4, Abdulaziz Abdulla AL Khulaifi2
Hamad Medical Corporation Heart Hospital, Qatar1, HMC Heart Hospital, Qatar2, Heart Hospital Hamad Medical Corporation, Qatar3, Hamad Medical Corporation (HMC), Doha, Qatar4,
Clinical Information
Patient initials or Identifier Number
A,I,
Relevant Clinical History and Physical Exam
Clinical report: A 58 y old male patient with no medical history of relevance, who was brought by ambulance complaining of severe central chest pain while he was
playing tennis, Pain started about 45 minutes before his arrival to the hospital. By examination he was in pain otherwise vitally stable, his blood pressure was 116/85 mmHg, heart rate was 54 beats/min.
Relevant Test Results Prior to Catheterization
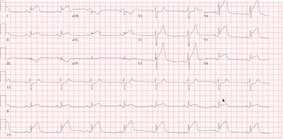
ECG showed ST elevation at anterolateral and posterior leads figure1, After loading him with Aspirin 300 mg and clopidogrel 300mg, Tenecteplase 45 mg
 figure3.avi
figure3.avi
figure4.avi
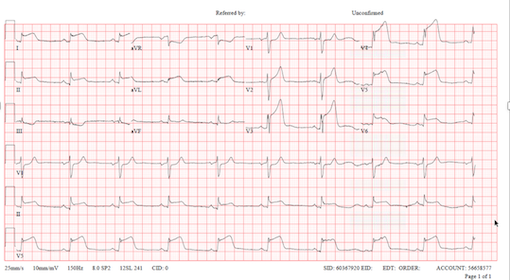
(for weight of 80 kg) intravenous bolus was given within 30 minutes of arrival. 90 minutes later ECG changes became more worse and chest pain didn’t
improve figure2.
Relevant Catheterization Findings
Rescue coronary angiography showed filling defects in the distal ( LAD) with 100% distal occlusion, OM3 proximal lesion of 50% with 100% distal
figure5.avi
figure6.avi
figure7.avi
occlusion, and RCA filling defect distally with TIMI II flow figure(5-6-7).
After wiring, the OM3 blood flow was restored then a 2.75 x 15mm Xience DES was deployed,
Interventional Management
Procedural Step
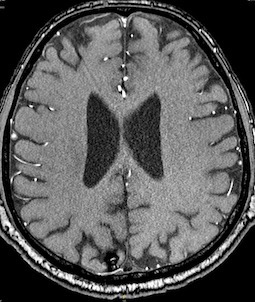
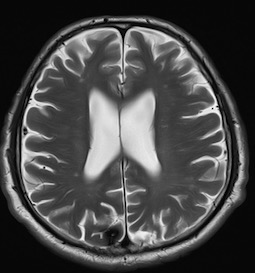
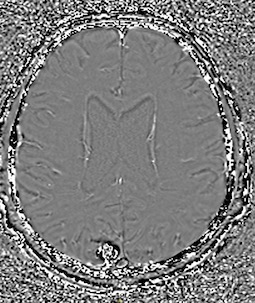
Transthoracic echocardiography was performed and showed a left atrial mass attached to the atrial septum figure(3-4). The mass was highly mobile, pedunculated with irregular surface measuring 2.5 cm in width and 1.7 cm in height. Left ventricular calculated ejection fraction was 40%, with RWMA.Patient was recommended for a surgical resection of the mass, however he refused the surgery. He was observed for 4 days then was discharged home in a stable condition. In less than 24 hours from discharge he presented to the emergency department with sudden onset of slurred speech. Neurologic examination was intact except from impressive aphasia. Head magnetic resonance (MRI) showed multiple small scattered bilateral acute infarcts with Chronic small hemorrhagic infarcts in both cerebral hemispheres and right cerebellar hemisphere (Figure 8-9-10). At this point he accepted the surgery, which was performed 10 days after the initial presentation. Cardiopulmonary bypass was established, the right atrium was opened longitudinally. The left atrium was entered through the fossa ovalis. The myxoma was very friable and could not be excised in one piece, it was excised with a part of the interatrial septum (IAS) which was closed with a pericardial patch. Echocardiography post-surgery showed no residual mass with no interatrial septum shunt, and calculated EF of 55%. Biopsy proved it to be a LA myxoma. Patient remained in the hospital for five days and discharged home in a stable condition.
Case Summary
This case indicates 1. that echocardiography better to be performed before coronary angiography when available in the context of an electrocardiogram showing ST elevation in multiple territories in a patient without cardiovascular risk factors. 2. The importance of prompt resection of myxoma whenever discovered especially when it is villous and small in size.