
Lots of interesting abstracts and cases were submitted for TCTAP 2022. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-001
"The Squid Game'- IVUS Guided Angioplasty in a Case of Spontaneous Coronary Artery Dissection Presenting With Ventricular Tachycardia Post COVID-19 Infection
By Mugilan Sundarajoo, Khin Maung Zan Mohd Saad Jalaluddin, Shaiful Azmi Yahaya
Presenter
Mugilan Sundarajoo
Authors
Mugilan Sundarajoo1, Khin Maung Zan Mohd Saad Jalaluddin2, Shaiful Azmi Yahaya3
Affiliation
National Heart Institute Ijn, Malaysia1, Hospital Pusrawi, Malaysia2, National Heart Institute, Malaysia3,
View Study Report
TCTAP C-001
CORONARY - Acute Coronary Syndromes (STEMI, NSTE-ACS)
"The Squid Game'- IVUS Guided Angioplasty in a Case of Spontaneous Coronary Artery Dissection Presenting With Ventricular Tachycardia Post COVID-19 Infection
Mugilan Sundarajoo1, Khin Maung Zan Mohd Saad Jalaluddin2, Shaiful Azmi Yahaya3
National Heart Institute Ijn, Malaysia1, Hospital Pusrawi, Malaysia2, National Heart Institute, Malaysia3,
Clinical Information
Patient initials or Identifier Number
448280
Relevant Clinical History and Physical Exam
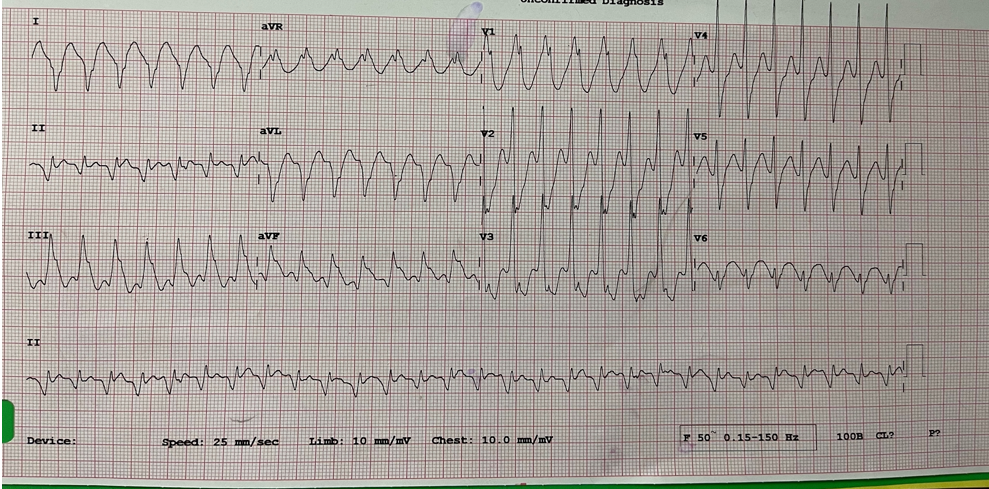
50-year-old male with no known coronary arterydisease and has well-controlled diabetes mellitus presented with palpitationsand shortness of breath. He has also just recovered from COVID-19 Category 2infection 2 weeks prior to presentation. ECG revealed ventricular tachycardia.Patient was in in respiratory distress upon presentation. BP-152/104,HR-174.
Relevant Test Results Prior to Catheterization
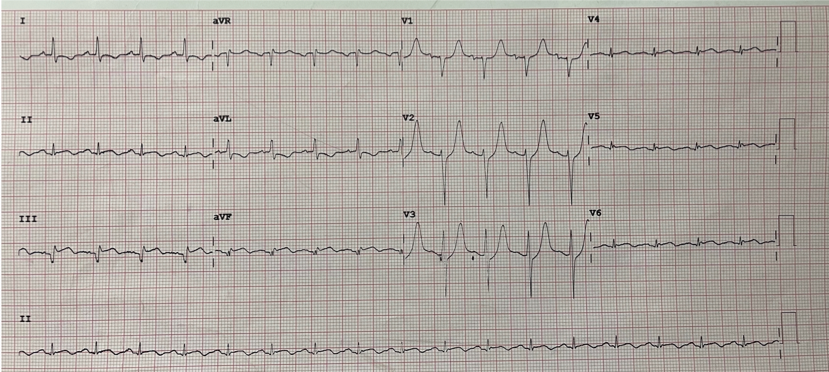
Chest X-ray was clear. Echocardiography globalhypokinesia with Ejection fraction of 35%. TAPSE- 1.7 cm, LVIDd- 5.3 cm andLVIDs- 4.0 cm Valves are normal. Patient was given IV Amiodarone 300mg stat andsubsequently cardioverted. Post cardioversion, ST elevation over inferior leadsis more evident and patient is symptomatic with chest pain and shortness ofbreath. He was brought to the catheterization lab for coronary angiogram.
Relevant Catheterization Findings
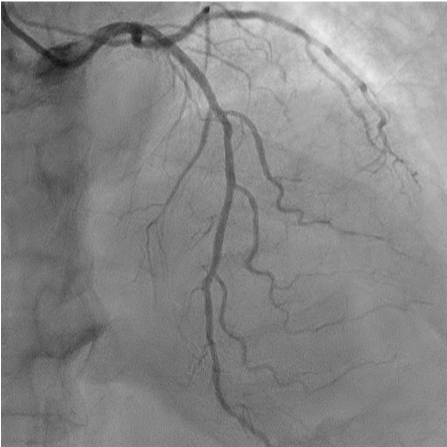
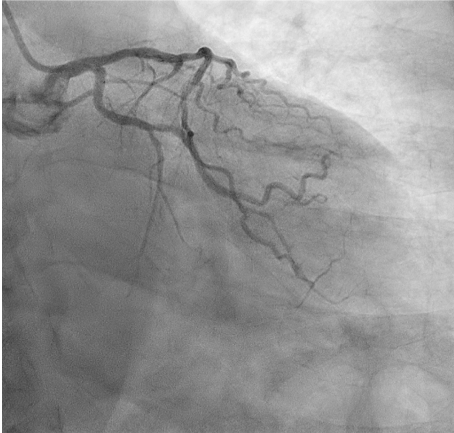
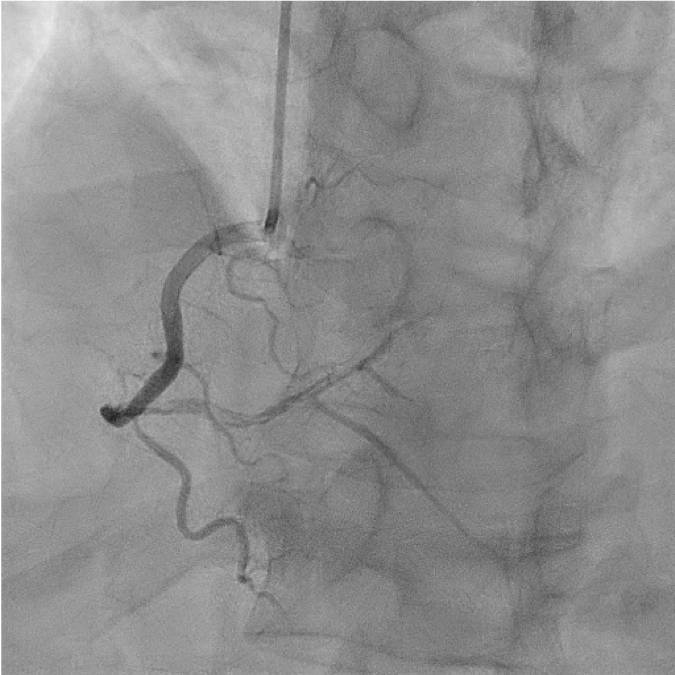
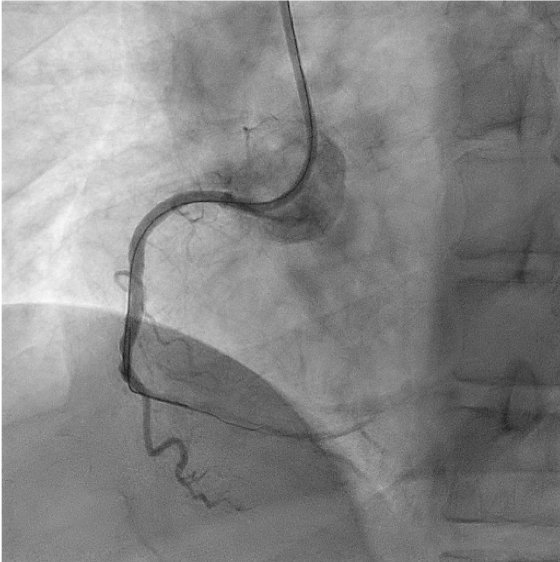
Coronary angiography revealed multiple linearfilling defects over mid to distal segment of RCA. LMS/LAD and LCX are free ofdisease.
Interventional Management
Procedural Step
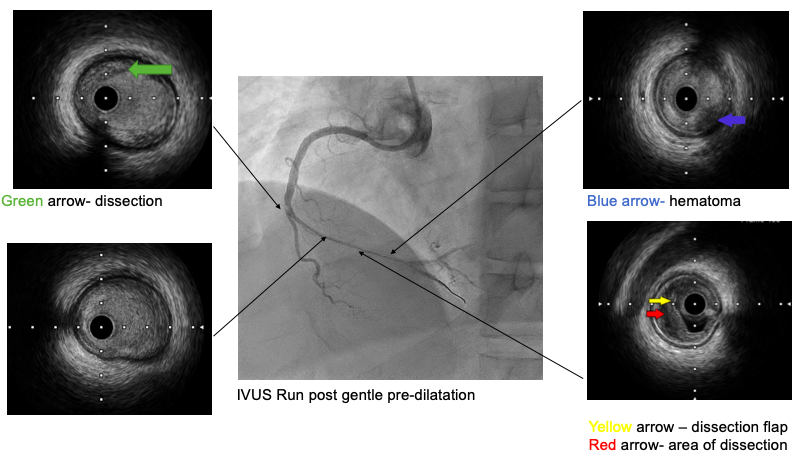
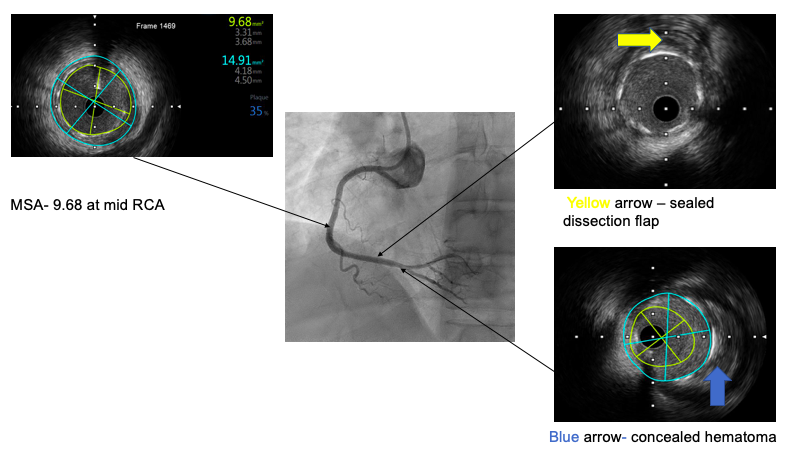
PCI done via right radial approach using 6FR SAL-1. Fielder- FC coronary guide wired down RCA but kept tracking into the falselumen. Using parallel wiring technique, Fielder- XT coronary guide wire waswired down the true lumen. IVUS imaging was attempted to further visualize thelesion in RCA for further intervention; however, IVUS catheter could not bepassed beyond the distal segment of RCA. Fielder XT subsequently wired down theRPDA branch assumed to be completely in the true lumen. Subsequently, there wasno-flow over the distal segment of RCA. Fielder XT was rewired again andFineCross Microcatheter aspiration confirmed that we were in the true lumen.This was ascertained further with IVUS. Sequential careful pre-dilatation wasdone using Semi Compliant Sapphire 3 1.5/15mm balloon and Sapphire 3 2.0/15mmat nominal pressure to rPL, RPDA and distal RCA. Further pre-dilatation of midto distal RCA with Sapphire 3 2.5/15 mm at 8 atm. 2.5/30 mm and 2.25/30 mm SequentPlease Neo Drug Coated Balloon deployed at the posterolateral and RPDA branchof RCA respectively. Xience Expedition 3.0/48 mm stent was deployed at 11 atmfrom the mid to distal RCA extending across the dissection flap. IVUS postangioplasty revealed well-opposed stents struts with good expansion and nostent edge dissection fulfilling all 3 IVUS criteria according to the Ultimatetrial. IVUS confirmed sealed dissection flap and concealed hematoma. Procedurewas uneventful otherwise and he was discharged well.
Case Summary
This is a rare presentation of Spontaneous CoronaryArtery Dissection in a middle-aged man post-COVID-19 infection involving theRCA who presented with ventricular tachycardia. PCI involving SCAD is verychallenging with high failure and complication rate. The decision torevascularize a dissected artery depends on both the coronary anatomy and thepatient’s clinical status. The use of intracoronary imaging, i.e., OCT or IVUSensures stent coverage and good wall apposition. For longer lesions, a multistepapproach with hybrid procedure like in our case (DES+ DCB) may be useful inpreventing IMH propagation and may promote positive vascular remodeling.