CVRF's Annual Meetings
----------------------------------------
2020
2019
2018
2017
2016
2015
2014
----------------------------------------
2019
----------------------------------------
2019
summitMD.com
CVRF.org
Meeting Information
Course Directors
Faculty
- International Faculty
- Korean Faculty
Focus
Scientific Program
• Meeting at a Glance
•
Program
- Main Arena
- Coronary Arena
- Endovascular Arena
- Symposium Arena
- Tutorial Arena
- Breakfast Meetings
- Satellite Symposia
- Oral Abstract Presentation
- Case Presentation
- Live Case Operators
- Conference for
Cardiovascular Nurse
& Technologist
- Cardiopulmonary
Rehabilitation Workshop
- Clinical Exercise
Specialist (CES) Workshop
Live Case Demonstration
E-Poster Abstracts
Live Case Transmission
Sites
Factoid
Syllabus
Summit Live Interview
Gallery
Daily Newspaper
Advance Registration
Housing
Exhibition
- Exhibition Information
- Exhibitor's List & Floor Plan
Learning Center
Eco-Friendly Convention
: Yes, Green!
Tour Information
- Korea, Sparkling
- About Seoul
- Visa
- Tour Program
Contact Us
About CVRF
2009 Brochure Download
Friday, April 24, 2009
Lessons from Four Late-Breaking Clinical Trials
Yesterday, there were 4 best abstract presentations at the Late-Breaking Clinical Trials session from 11:50 AM to 12:30 PM at the Main Arena.
Randomized Comparison of Primary Percutaneous Coronary Intervention with Combined Proximal Embolic Protection and Thrombus Aspiration versus Primary Percutaneous Coronary Intervention Alone in ST-segment Elevation Myocardial Infarction.
Dr. Karel Koch
Embolization during primary percutaneous coronary intervention (PCI) for ST-segment elevation myocardial infarction (STEMI) may result in microvascular obstruction, reduced myocardial per fusion, and impaired prognosis. Dr. Karel Koch from Academic Medical Center, University of Amsterdam, Netherlands, introduced a
novel approach of preventing embolization, the Proxis system (St. Jude Medical, St Paul, MN, USA), which combines proximal embol ic protect ion and thrombus aspiration during primary PCI.
Following urgent angiography, Dr. Karel Koch, et al, randomized 284 patients between pr imary PCI wi th the Proxis system or primary PCI alone. The primary endpoint was complete (70%) ST-segment resolution(STR),
evaluated in a blind-ed manner at an independent core laboratory.
Complete STR at time of last contrast occurred in 66% of patients receiving combined proximal embolic protection and aspiration and in 50% of control patients (absolute difference, 16.3% [95% confidence interval, 4.3% to 28.2%]; P=0.009).The difference between the 2 groups in the rate of complete STR was statistically significant. The mean percent STR at last contrast in both arms was also stat ist ical ly signi ficant ly different (73.2% vs. 63.4%, respectively; P=0.009) . A signi f icant ly lower STsegment curve areaI........
Case Presentation with Experts Review
This year, the Challenging case competition with experts' review session has more extended to give opportunities for physicians at the Coronary and Endovascular arena and will be held from 8:30 AM-4:30 PM on April 24 and there will be presented about 80 cases from all over the world.
A Retrograde Approach for the RCA CTO Lesion with Severe Calcification
Dr. Tadashi Kikuchi
A 52-year old male presented with a 1-month history of chest pain on effort. Echocardiography revealed normal left ventricular contractility without RWMA. Stress electrocardiography showed 2-3mm ST depression in leads V3 to V6 leads during low workload. Left coronary angiogram (LCA) showed a 90% stenosis of the mid LCX. Right coronary angiogram (RCA) showed 99% stenosis of the proximal RCA and CTO of the mid RCA with severe calcification, but with good collateral flow from the LAD. Dr. Kikuchi recommended CABG. The patient and his family however refused CABG. In order to overcome the severe LCX calcification, Rota-ablation was performed
with the 1.5mm burr. Pre-dilatation was performed with 2.5mm balloon, after which a Cypher stent (3.0X33mm; 20atm) was deployed in the calcified LCX lesion.
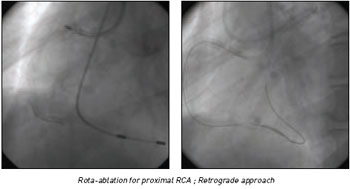
Seven days later, PCI for CTO of the RCA by antegrade approach; Rota wire was placed into the mid RCA. Rota-ablation to the proximal RCA was performed with 1.5mm
burr. Pre-dilation was performed with 2.5 X 15 mm Maverick, after which a Cypher stent (3.5 X 23 mm) was deployed at the proximal RCA lesion. Subsequently, antegrade CTO recanalization was attempted. But, an antegrade guide wire (Miracle 3g) was introduced into the subintima space. So the antegrade approach was abandoned and a
retrograde approach was tried.
PCI for CTO of the RCA by retrograde approach; A Fielder FC wire with microcatheter was successfully introduced into the distal RCA through the collateral channel between the septal branch and the RCA. The microcatheter was pulled......












 Yesterday,
there were 4 best abstract presentations at the Late-Breaking Clinical Trials
session from 11:50 AM to 12:30 PM at the Main Arena.
Yesterday,
there were 4 best abstract presentations at the Late-Breaking Clinical Trials
session from 11:50 AM to 12:30 PM at the Main Arena.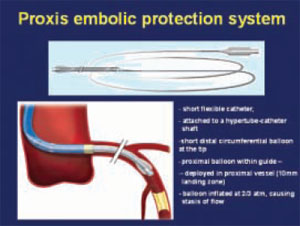 Following
urgent angiography, Dr. Karel Koch, et al, randomized 284 patients between
pr imary PCI wi th the Proxis system or primary PCI alone. The primary endpoint
was complete (70%) ST-segment resolution(STR),
Following
urgent angiography, Dr. Karel Koch, et al, randomized 284 patients between
pr imary PCI wi th the Proxis system or primary PCI alone. The primary endpoint
was complete (70%) ST-segment resolution(STR),
 A 52-year old male
presented with a 1-month history of chest pain on effort. Echocardiography
revealed normal left ventricular contractility without RWMA. Stress electrocardiography
showed 2-3mm ST depression in leads V3 to V6 leads during low workload.
Left coronary angiogram (LCA) showed a 90% stenosis of the mid LCX. Right
coronary angiogram (RCA) showed 99% stenosis of the proximal RCA and CTO
of the mid RCA with severe calcification, but with good collateral flow
from the LAD. Dr. Kikuchi recommended CABG. The patient and his family however
refused CABG. In order to overcome the severe LCX calcification, Rota-ablation
was performed
A 52-year old male
presented with a 1-month history of chest pain on effort. Echocardiography
revealed normal left ventricular contractility without RWMA. Stress electrocardiography
showed 2-3mm ST depression in leads V3 to V6 leads during low workload.
Left coronary angiogram (LCA) showed a 90% stenosis of the mid LCX. Right
coronary angiogram (RCA) showed 99% stenosis of the proximal RCA and CTO
of the mid RCA with severe calcification, but with good collateral flow
from the LAD. Dr. Kikuchi recommended CABG. The patient and his family however
refused CABG. In order to overcome the severe LCX calcification, Rota-ablation
was performed

