
Lots of interesting abstracts and cases were submitted for TCTAP 2023. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-105
A 'Tsunami' Consequence of Intravascular Lithotripsy Balloon Rupture - Extensive Coronary Artery Dissection With Intramural Hematoma
By Chi Na Cheng
Presenter
Chi Na Cheng
Authors
Chi Na Cheng1
Affiliation
Pok Oi Hospital, Hong Kong, China1,
View Study Report
TCTAP C-105
CORONARY - Complications (Coronary)
A 'Tsunami' Consequence of Intravascular Lithotripsy Balloon Rupture - Extensive Coronary Artery Dissection With Intramural Hematoma
Chi Na Cheng1
Pok Oi Hospital, Hong Kong, China1,
Clinical Information
Patient initials or Identifier Number
Yip SC
Relevant Clinical History and Physical Exam
61-year-old gentlemanExsmokerhypertensionDiabetes mellitus type 2End-stage renal failure on hemodialysis. Presented with recurrent chest discomfort during hemodialysis. Physical examination was unremarkable
Relevant Test Results Prior to Catheterization
Echocardiography showed a impaired left ventricular systolic function, with an ejection fraction of 37% by simpson biplane. There was hypokinesia over inferior, inferolateral and lateral walls
Relevant Catheterization Findings
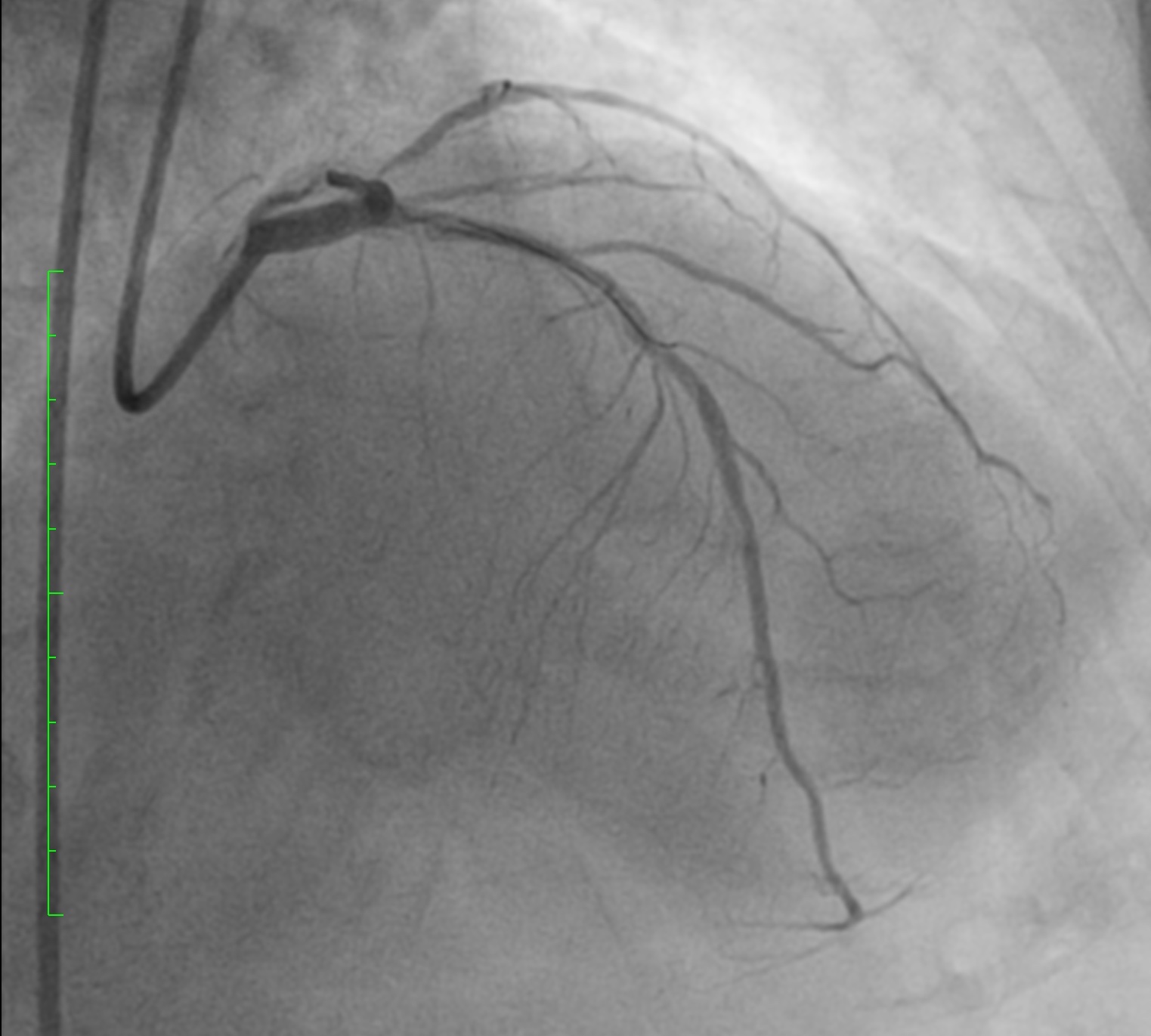
LMS: normalLAD: heavily calcified. ostial-mLAD diffuse severe disease with maximal 80% stenosis. D1 severe disease
LCx: mLCx subtotal occlusion. dLCx diffuse severe disease. ostial OM1 90% stenosisRCA: Dominant, mRCA diffuse severe disease with maximal 90% stenosis. dRCA 80% stenosis
LCx: mLCx subtotal occlusion. dLCx diffuse severe disease. ostial OM1 90% stenosisRCA: Dominant, mRCA diffuse severe disease with maximal 90% stenosis. dRCA 80% stenosis
Interventional Management
Procedural Step
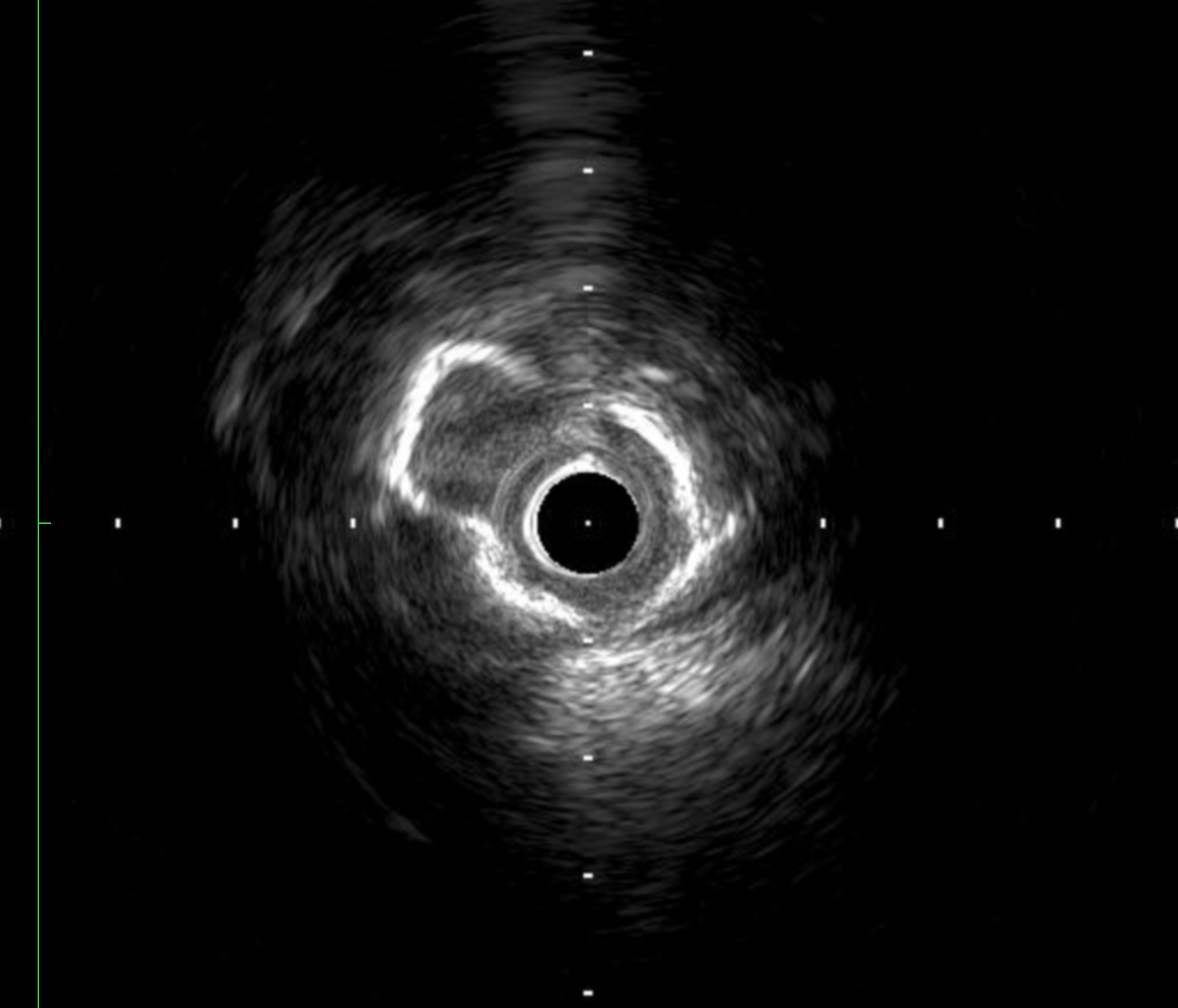
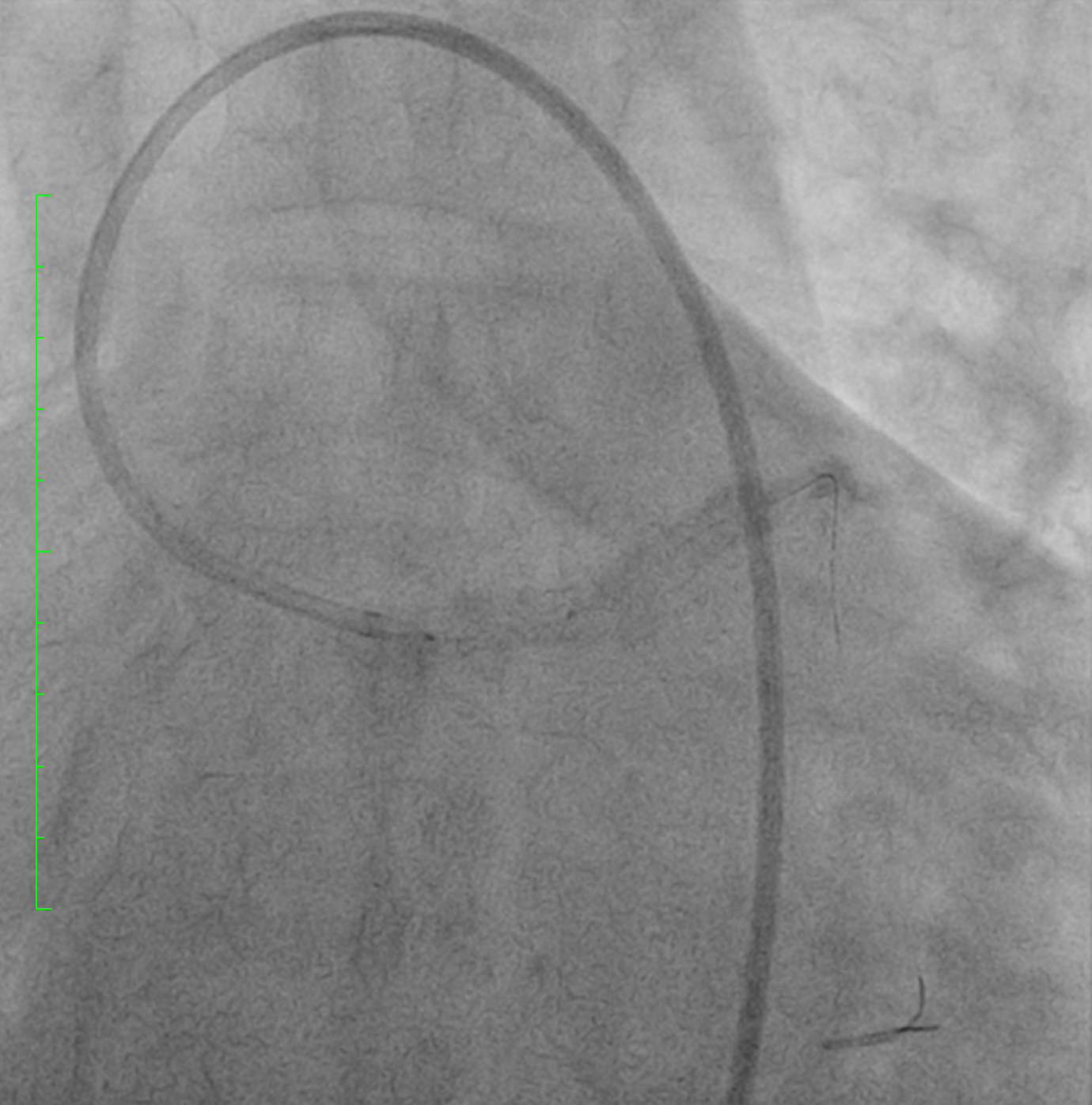
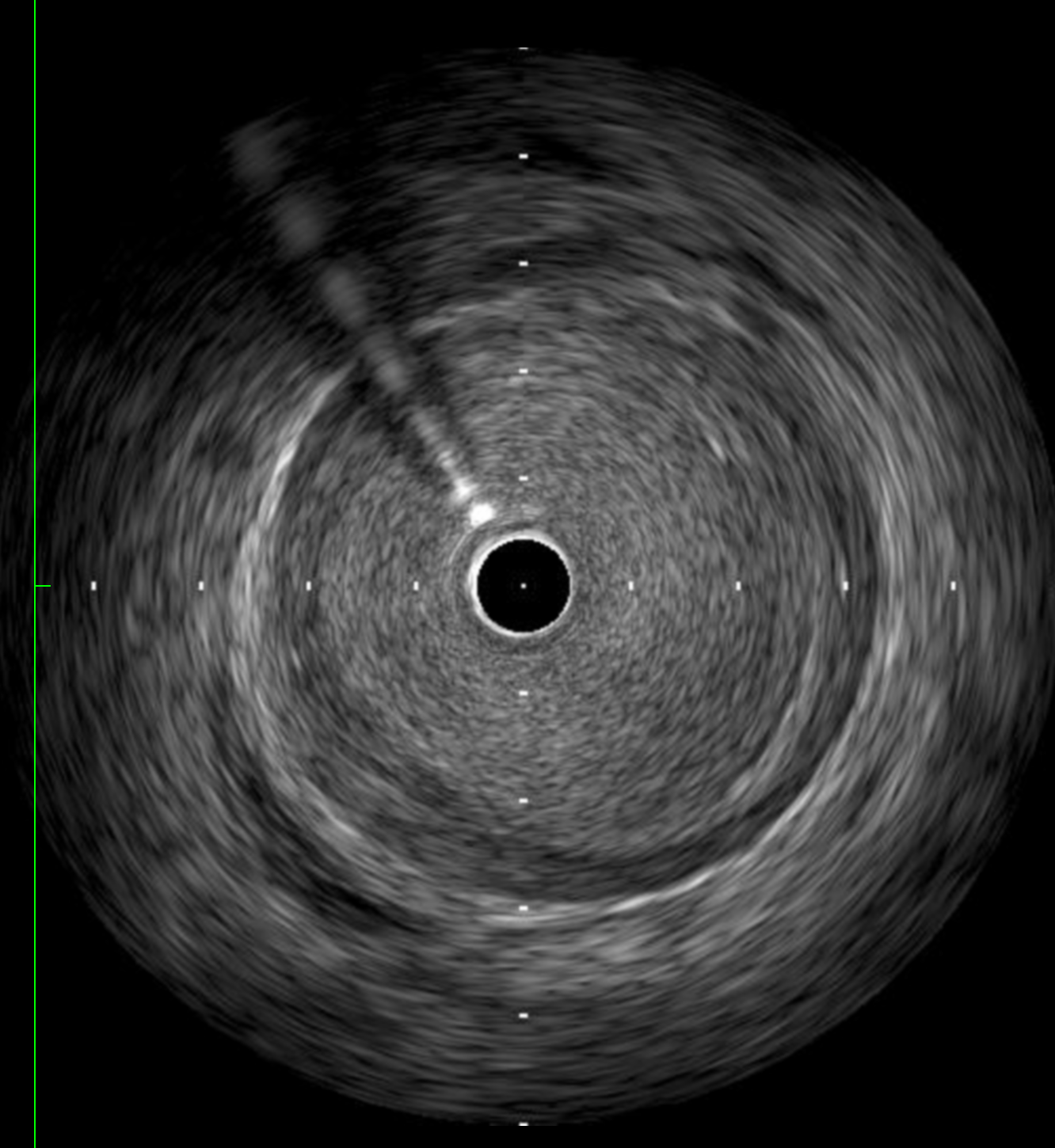
We decided to modify the calcium using intravascular lithotripsy (IVL) before stenting. Lithoplasty balloon was inflated at 4 atm at mLAD. Balloon ruptured during the first pulse of shockwave, leading to a type C dissection from left main stem (LMS) to proximal LAD (pLAD). IVUS was used to evaluate the LAD, which showed extensive dissection and intramural hematoma (IMH) from distal LAD up to LMS. We successfully deployed a 5.0x12mm drug-eluting stent (DES) at LMS. IVUS showed good stent expansion and apposition of the stent, with small amount of IMH noted behind the stent. Predilation of proximal to mid LAD (p-mLAD) was done using 3.0x15mm balloon. Another 2.5x38mm DES was deployed to mid to distal LAD (m-dLAD). Post-dilation to m-dLAD was done with a 3.0x15 balloon. A third DES (3.5x34mm) was advanced to p-mLAD with a 6 Fr guide extension catheter. Post-dilation to p-mLAD was done with a 3.5x15mm balloon. LMS was further post-dilated using a 5.5x8mm balloon. 7 Fr IL 3.5 guiding catheter was used to engaged the RCA. Mid RCA (mRCA) was predilated using a 2.0x15mm balloon. IVUS was used for interrogation. Total 10 therapy of IVL therapy was delivered to mRCA. A DES (3.5x38mm) was deployed to mid to distal RCA. Another DES (4.0x23mm) was deployed to proximal to mid RCA (p-mRCA). Post dilation to p-mRCA was done with 3.5x15mm balloon.
Case Summary
Literature on the mechanisms of IVL-related complications are scarce. Lee Tjen Jhung et al. proposed the possible mechanisms of IVL-related dissection to be (i) luminally protruding nodular calcium (ii) significant tortuosity of calcified coronary lesions, and (iii) possible gaps in contact between the balloon and luminal wall.
In our case, we postulated that the lithotripsy therapy caused crack in the calcified lesion, which may create high focal pressure onto the balloon body, which caused balloon rupture. The high pressure generated during balloon rupture in mid LAD caused extensive dissection and intramural hematoma from distal LAD up to LMS.
In our case, we postulated that the lithotripsy therapy caused crack in the calcified lesion, which may create high focal pressure onto the balloon body, which caused balloon rupture. The high pressure generated during balloon rupture in mid LAD caused extensive dissection and intramural hematoma from distal LAD up to LMS.