
Lots of interesting abstracts and cases were submitted for TCTAP 2023. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-129
My First Perforation and How I Treated! Why Important to Know Using of Coils (Self-Made) In Bail Out Situation (Perforation-Treating, Next Perforation-Treating and Again Perforation)
By Najmiddin Makhkamov, Javokhir Anvarov
Presenter
Najmiddin Makhkamov
Authors
Najmiddin Makhkamov1, Javokhir Anvarov1
Affiliation
Fedorovich Klinikasi LLC, Uzbekistan1,
View Study Report
TCTAP C-129
CORONARY - Complications (Coronary)
My First Perforation and How I Treated! Why Important to Know Using of Coils (Self-Made) In Bail Out Situation (Perforation-Treating, Next Perforation-Treating and Again Perforation)
Najmiddin Makhkamov1, Javokhir Anvarov1
Fedorovich Klinikasi LLC, Uzbekistan1,
Clinical Information
Patient initials or Identifier Number
Patient K.G. ID 408
Relevant Clinical History and Physical Exam
Female 71 y.o.
Relevant Test Results Prior to Catheterization
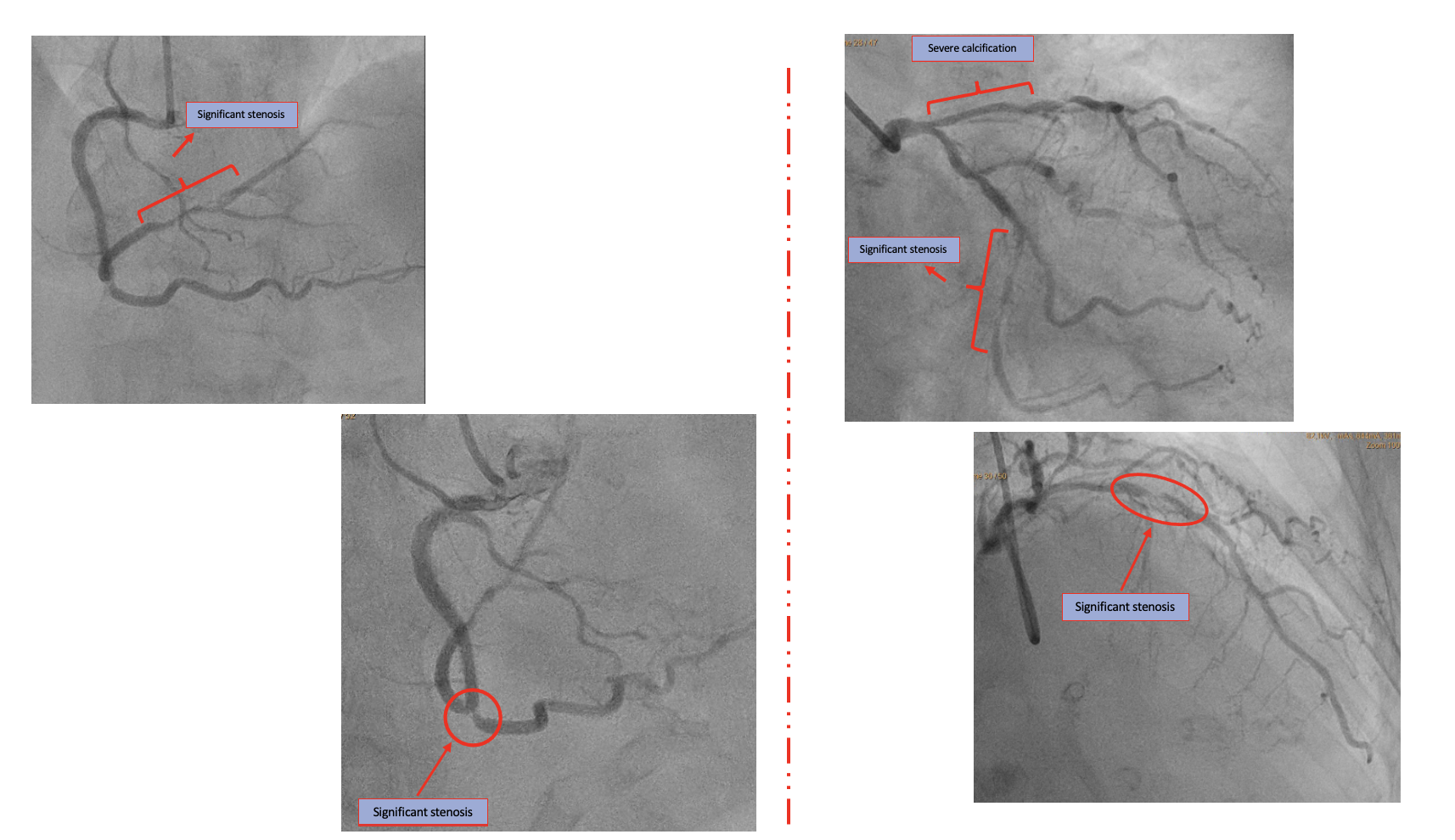
Relevant Catheterization Findings
LM bifurcation stenosis - 30-50% (Medina 1:1:1). LAD - severe calcification and significant stenosis - 90% of middle part. LCX - severe calcification and significant stenosis - 80% of distal part. RCA - significant ostial stenosis. In middle part significant stenosis - 85%. PDA - middle part stenosis - 80%. Before implanted stents are without in-stent restenosis.
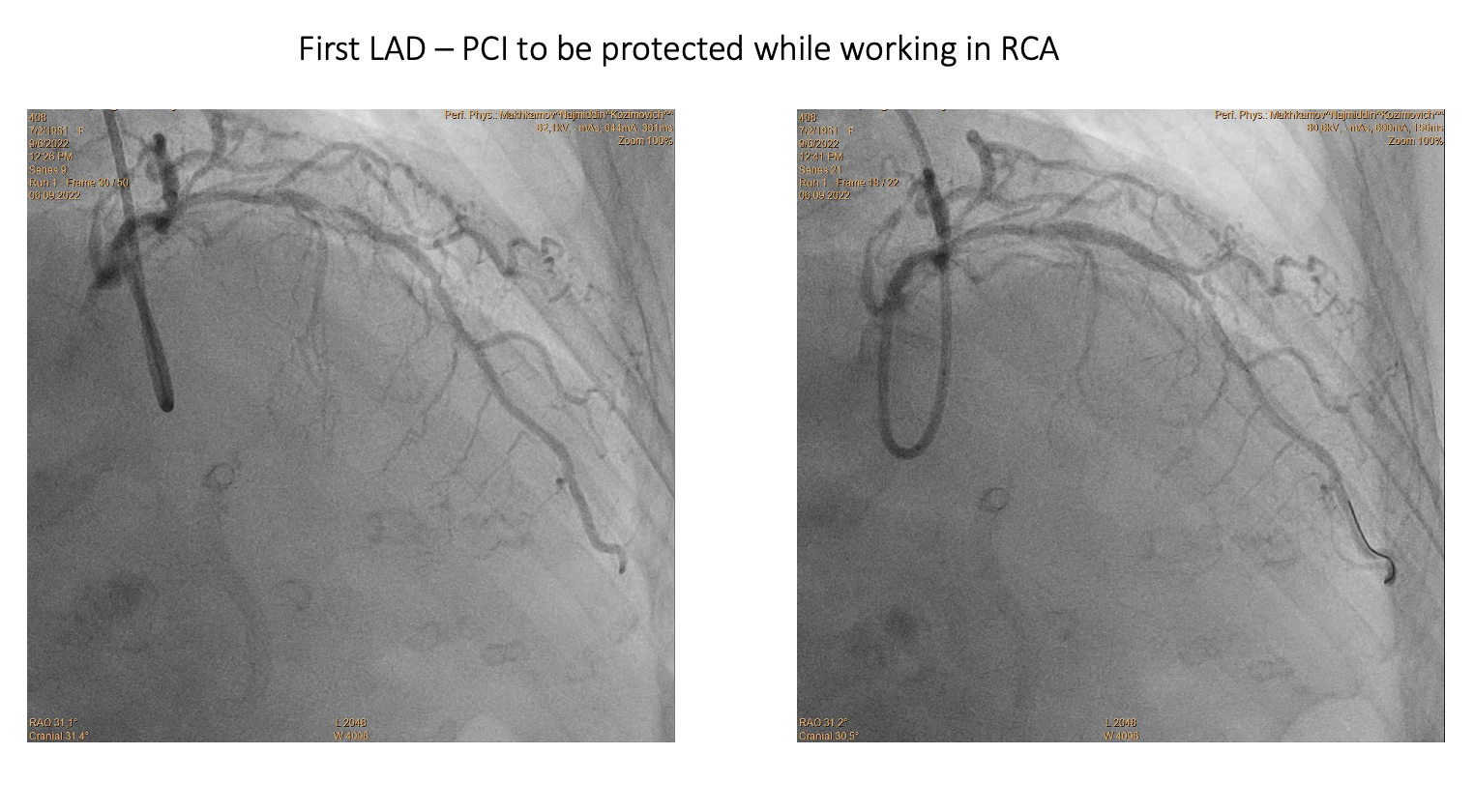
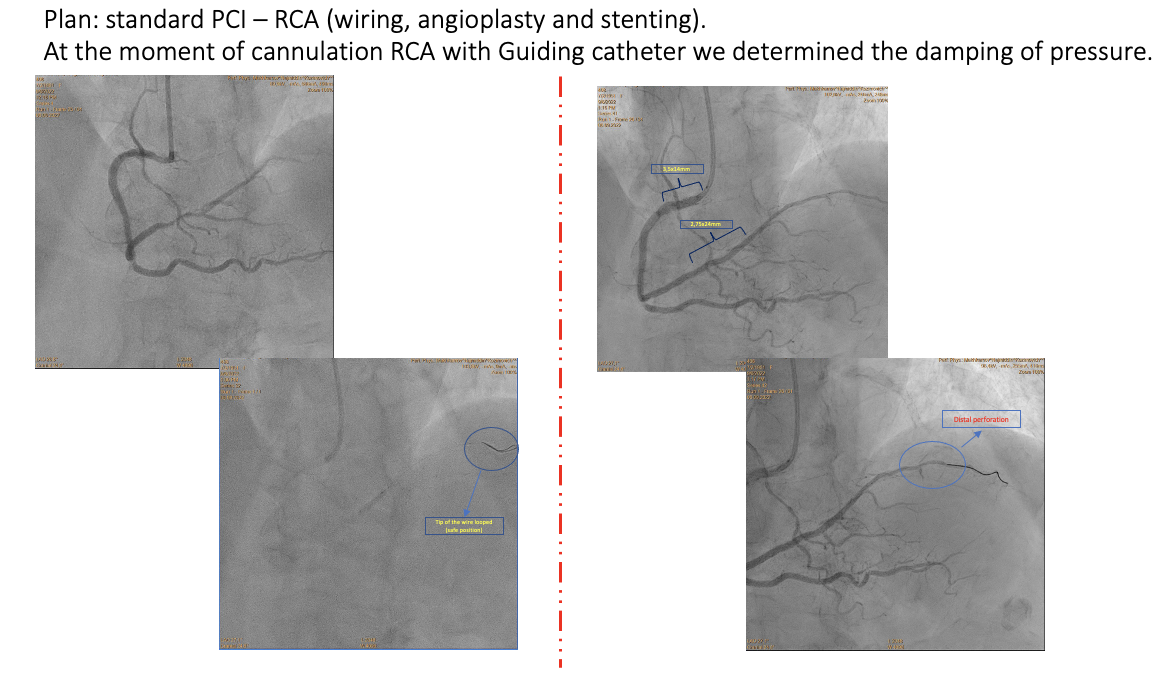
Interventional Management
Procedural Step
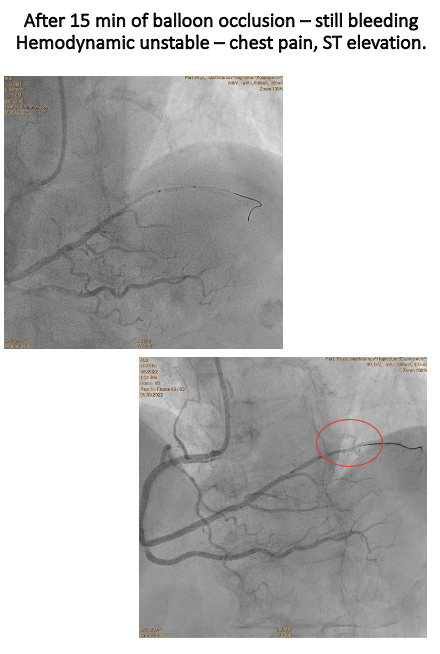
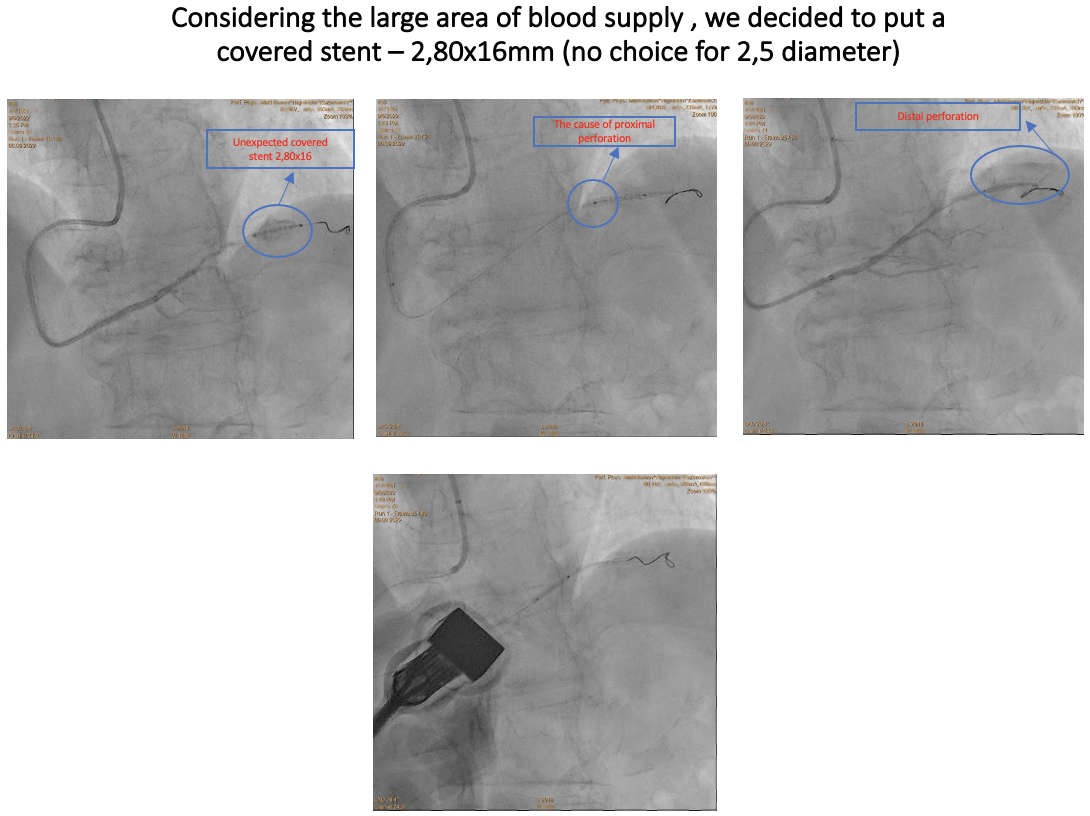
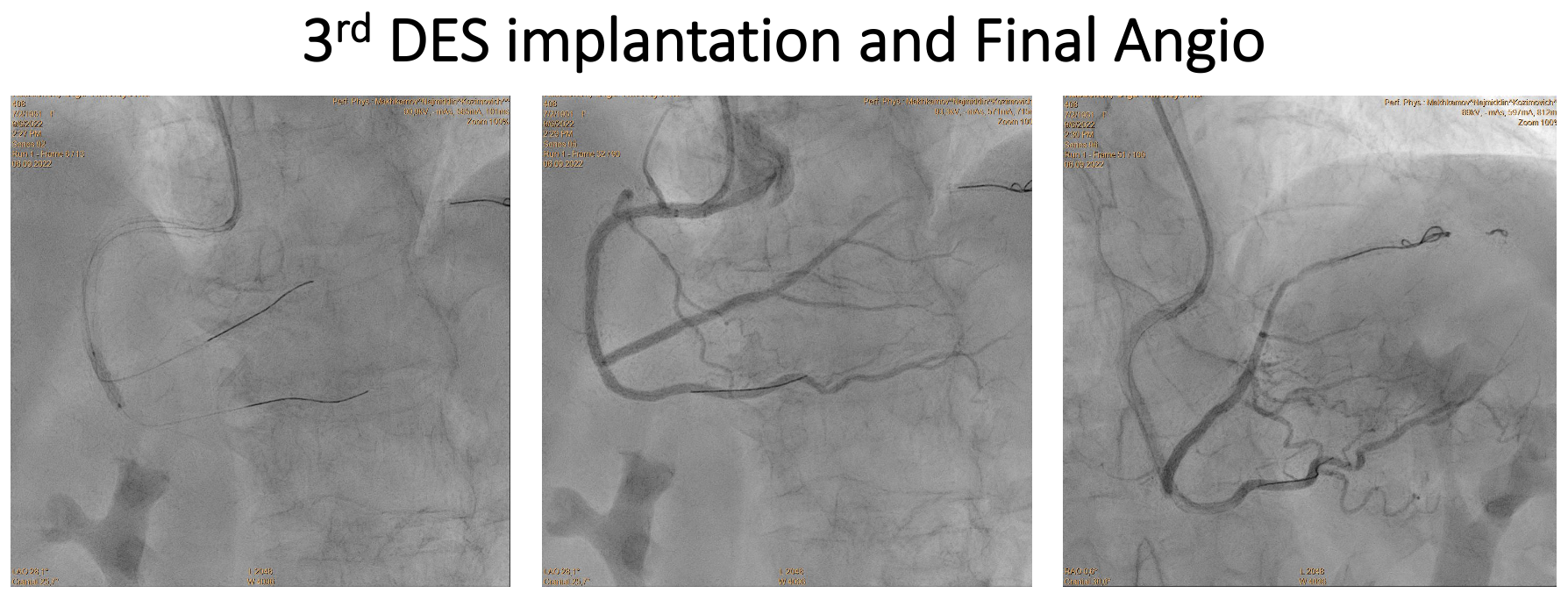
What’s next?
Case Summary
1) Never underestimate “simple” lesions