
Lots of interesting abstracts and cases were submitted for TCTAP 2023. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-146
Save the Day for the Complications of Endovascular Treatment
By Heng-You Sung, Chun-Wei Lee
Presenter
Heng-You Sung
Authors
Heng-You Sung1, Chun-Wei Lee2
Affiliation
Mackay Memorial Hospital Tamsui Branch, Taiwan1, Mackay Memorial Hospital, Taiwan2,
View Study Report
TCTAP C-146
ENDOVASCULAR - Complications (Endovascular)
Save the Day for the Complications of Endovascular Treatment
Heng-You Sung1, Chun-Wei Lee2
Mackay Memorial Hospital Tamsui Branch, Taiwan1, Mackay Memorial Hospital, Taiwan2,
Clinical Information
Patient initials or Identifier Number
38386675
Relevant Clinical History and Physical Exam
80 years old womanPast Medical History: HTN, T2DM, Dyslipidemia, CKD stage 3PAD s/p PTA, s/p stenting, 3 years agoT11 compression fracture s/p percutaneous vertebroplasty, 2021/10/21Left OA knee s/p TKA, 2016/04/18Chief Complaint: bilateral lower limbs numbness and pain intermittently for 3 months
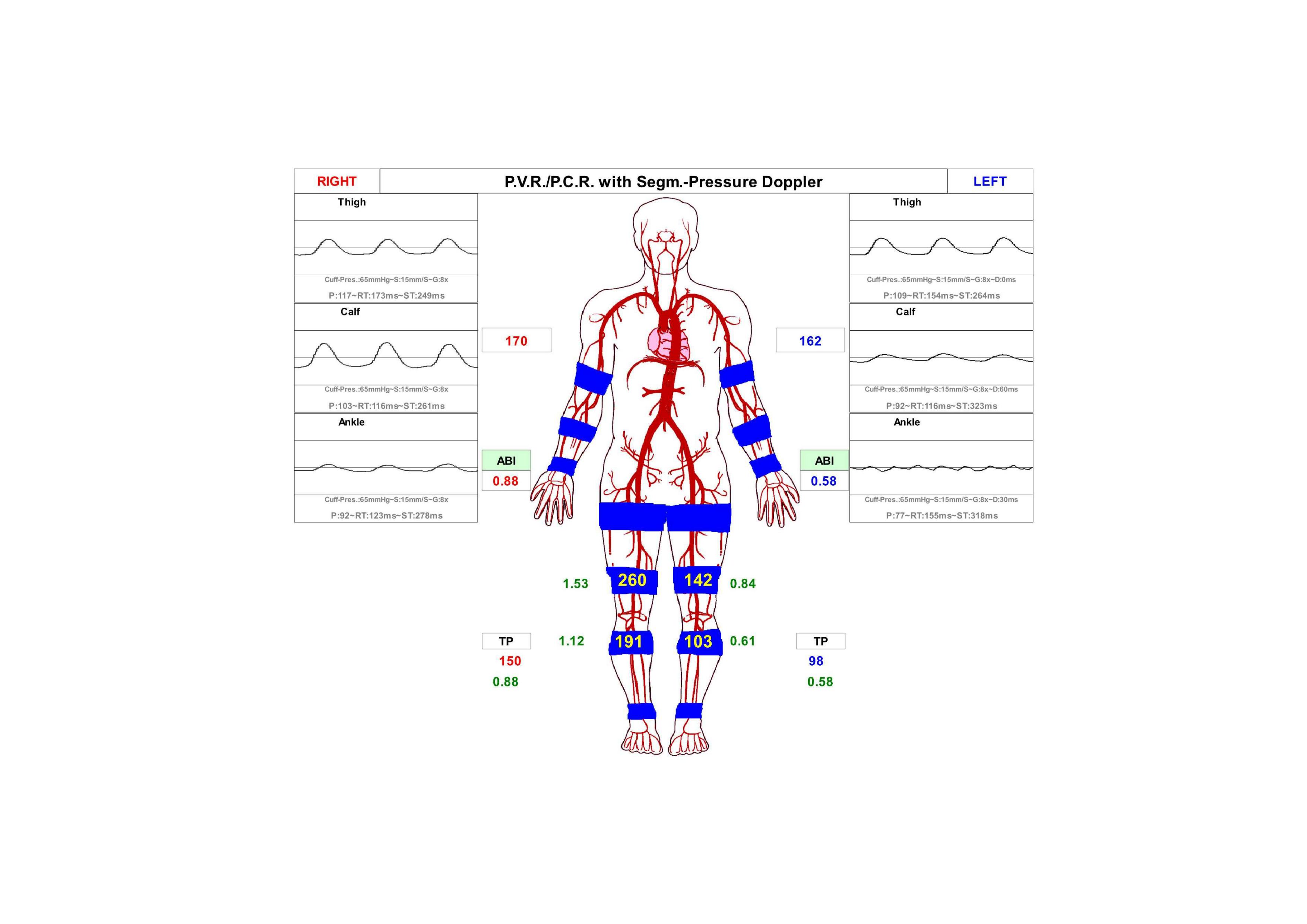
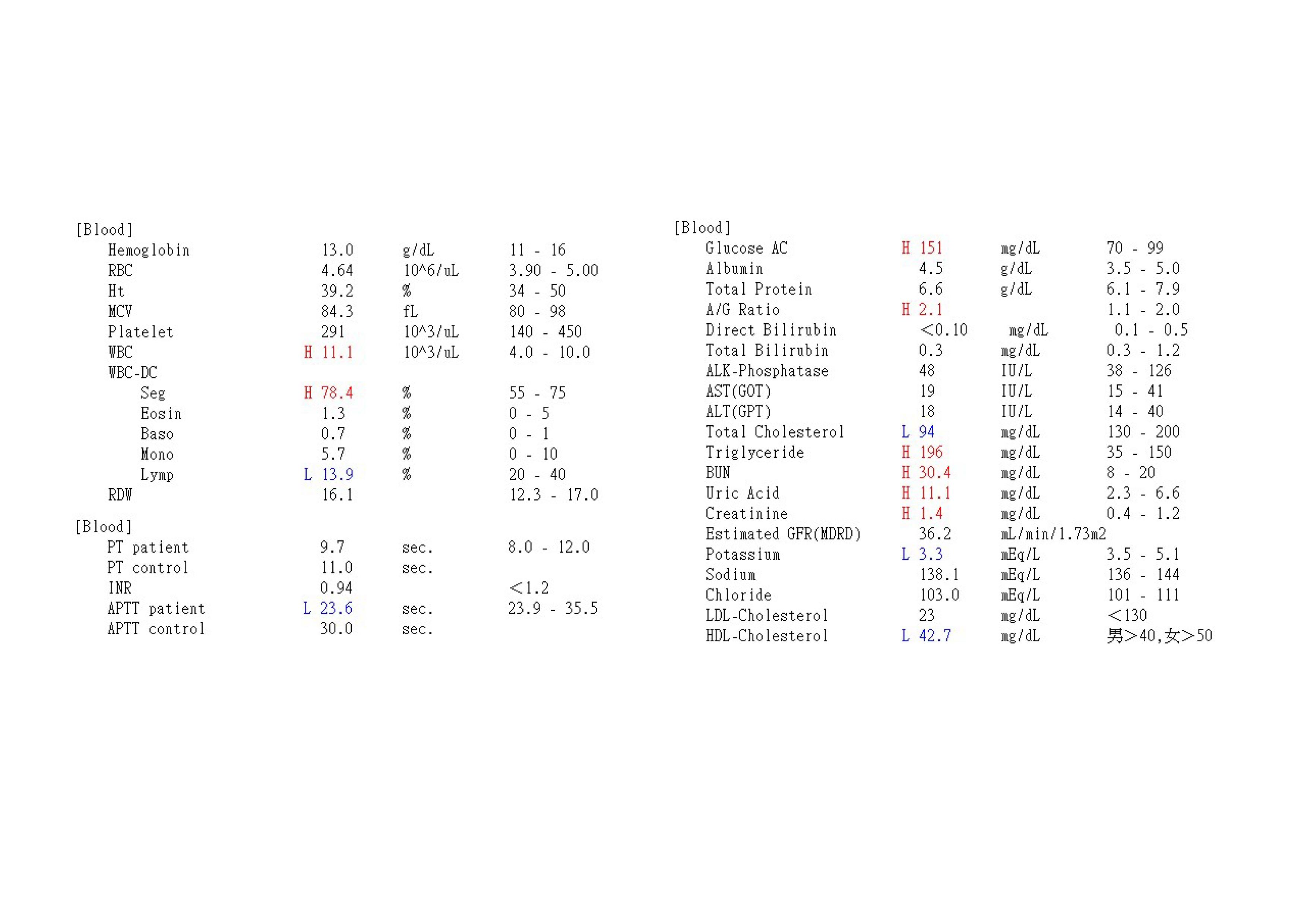
Relevant Test Results Prior to Catheterization
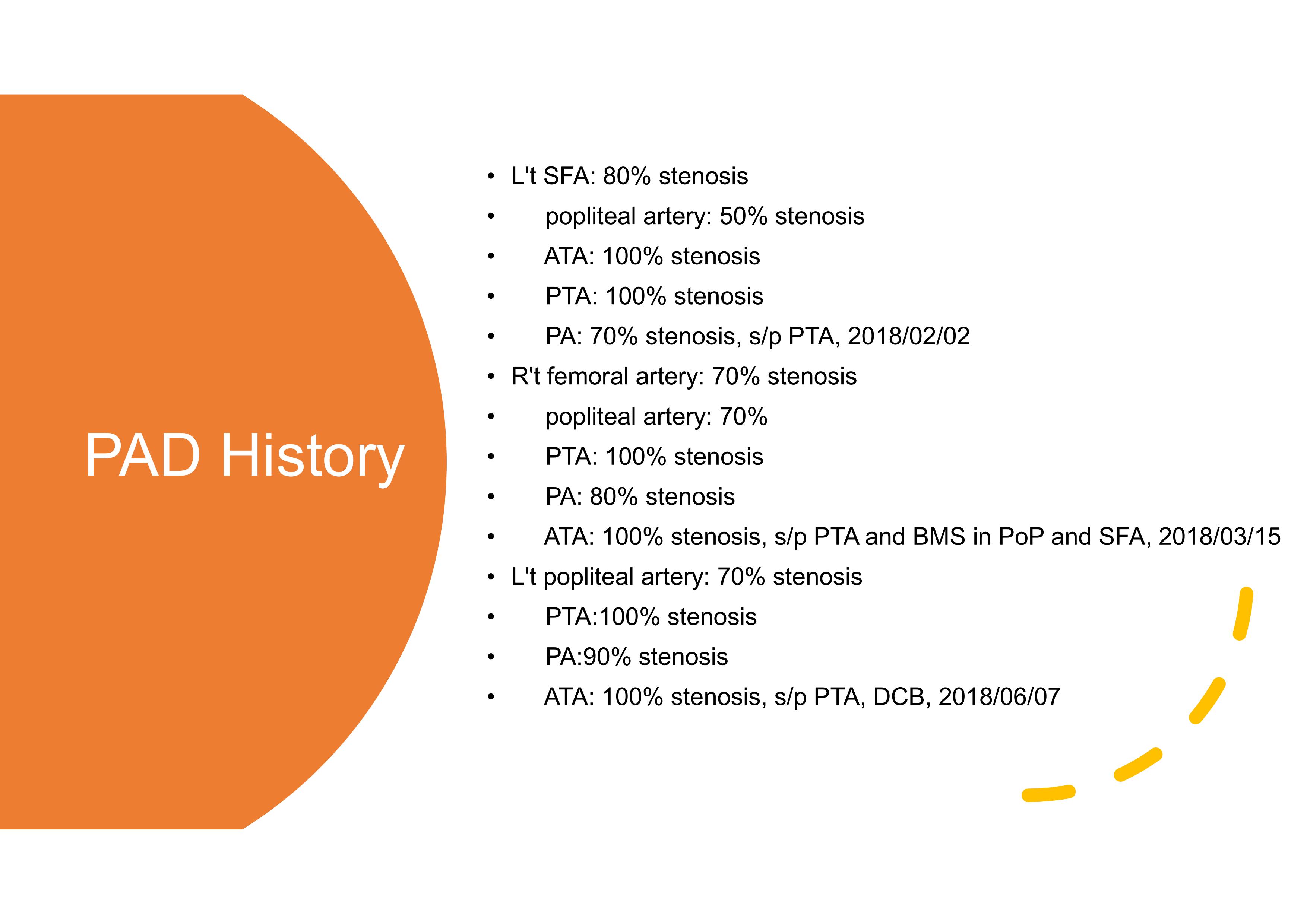
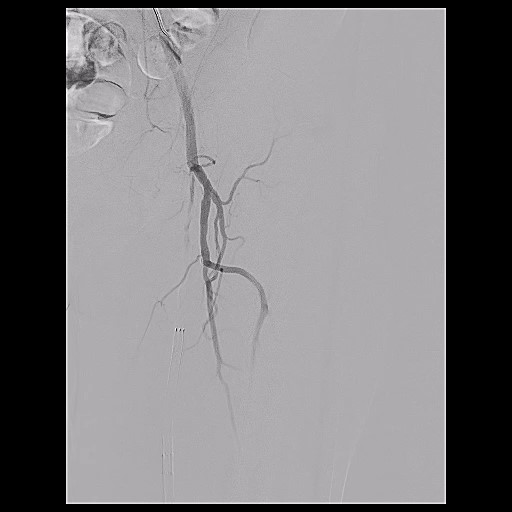
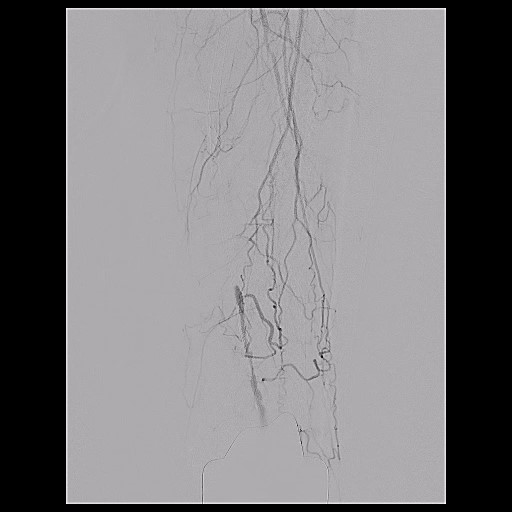
Relevant Catheterization Findings
Left SFA 100% stenosisLeft popliteal artery: 70% stenosisLeft ATA: 100% stenosisLeft PTA: 70% StenosisLeft PA: 70% Stenosis
Interventional Management
Procedural Step
Transfemoral approach: L`t Common femoral a. with 6 Fr Ansel sheath antegrade puncture.1. We tried to advance Passeo 6*80*80 balloon catheter with 0.018 connect wire, but failed due to steep angle and prolapse of sheath.2. We changed connect wire to Terumo stiff wire via Passeo 6*80*80 balloon catheter.3. We change 6Fr ansel sheath to 6F Destination long sheath.
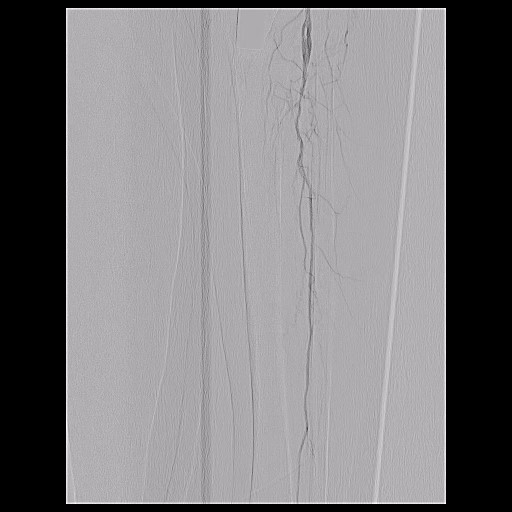
PTA for Left Superficial femoral artery1. We used Paseeo 6.0*80mm*80cm supporting catheter with tried antegrade approach and successfully go through L't PA.2. POBA with Passeo 6*80*80 in Left SFA and 5*80*80 in Left SFA instent up to 7 atm.3. POBA with Passeo 2.5*80*130 up to 14 atm in Left POP to PA.4. POBA with Passeo 6*150*130 up to 6 atm in left SFA5. EVERFLEX 6*120 was deployed in Left SFA.6. DCB with Passeo Lux 4*120*130 balloon catheter in Left SFA to POP instent.7. DCB with Passeo Lux 6*120*130 balloon catheter in Left SFA.8. We changed left radial artery sheath to 6Fr sheath.9. We advanced EUCA PW 6*80*135 balloon catheter via left radial artery to left common femoral artery.10. We removed Destination sheath and inflate EUCA PW 6*80*135 balloon catheter in Left SFA to internal compression to puncture site.11. External compression for hemostasis was also applied.12. We check final angiography and showed no extravasation over left femoral artery.
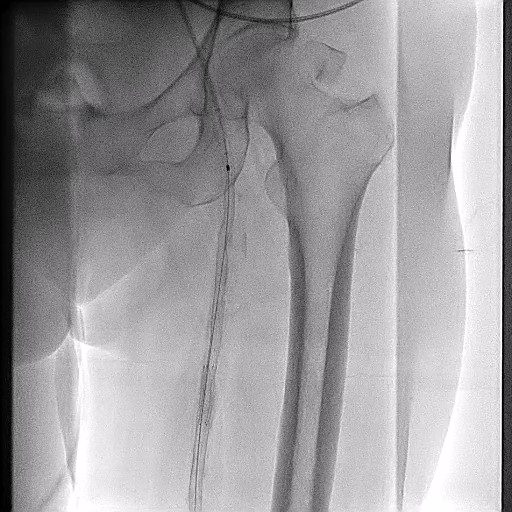

PTA for Left Superficial femoral artery1. We used Paseeo 6.0*80mm*80cm supporting catheter with tried antegrade approach and successfully go through L't PA.2. POBA with Passeo 6*80*80 in Left SFA and 5*80*80 in Left SFA instent up to 7 atm.3. POBA with Passeo 2.5*80*130 up to 14 atm in Left POP to PA.4. POBA with Passeo 6*150*130 up to 6 atm in left SFA5. EVERFLEX 6*120 was deployed in Left SFA.6. DCB with Passeo Lux 4*120*130 balloon catheter in Left SFA to POP instent.7. DCB with Passeo Lux 6*120*130 balloon catheter in Left SFA.8. We changed left radial artery sheath to 6Fr sheath.9. We advanced EUCA PW 6*80*135 balloon catheter via left radial artery to left common femoral artery.10. We removed Destination sheath and inflate EUCA PW 6*80*135 balloon catheter in Left SFA to internal compression to puncture site.11. External compression for hemostasis was also applied.12. We check final angiography and showed no extravasation over left femoral artery.
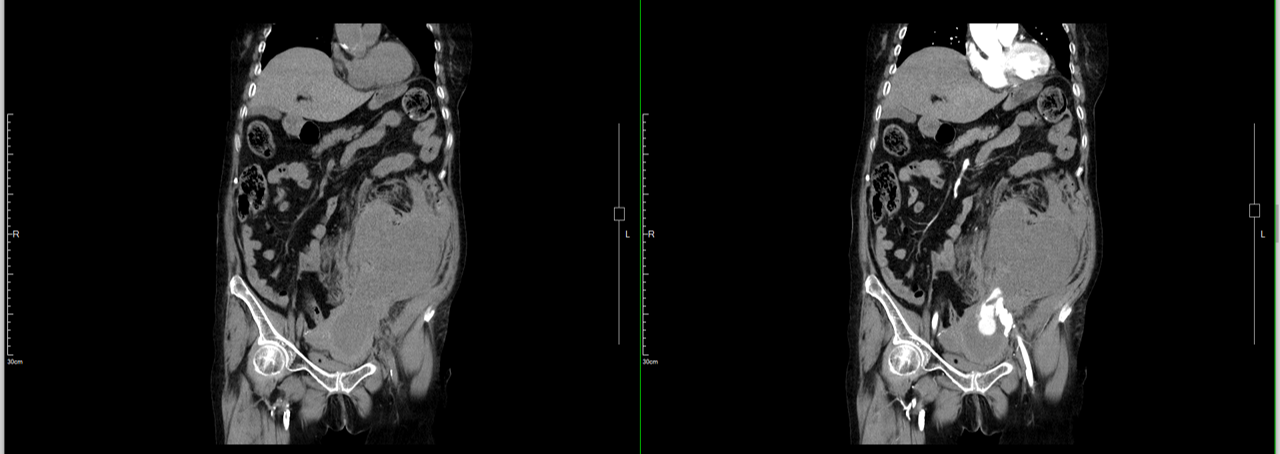
The patient then had shortness of breath, and hypotension
The CT showed extravasation from left common femoral artery and retroperitoneal hematoma
Case Summary
1. REEF 8.0*20mm*80cm supporting catheter tried retrograde approach through left common iliac artery2. Predilatation, REEF 8.0*20mm, 8-8 atm.3. Assurant 8.0*30mm*80cm stent, left common iliac artery at 8 atm.4. Postdilatation, REEF 8.0*20mm*80cm, 10-10 atm.5. VIABAHN 7.0*5mm*80cm stent, left external iliac artery 6. Angiography showed no further extravasation.7. The patient could tolerate the procedure. 8. Antegrade approach, 0.018 wire through left SFA.9. POBA, Passeo18 balloon 40*150mm, 6-8-14-14 atm.10. The patient could tolerate the procedure.Retroperitoneal HemorrhageInfrequent but seriousHigh access/non-compressible access siteCovered Stent as Salvation in the Last Resort!