
Lots of interesting abstracts and cases were submitted for TCTAP 2023. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-030
Native Vessel or Graft Occlusion- Dilemma of Identifying the Culprit Vessel of Inferior Wall ST Elevation Myocardial Infarction in a Post Coronary Artery Bypass Graft Patient
By Jegan Sivalingam, Mathavan Alagarsamy
Presenter
Jegan Sivalingam
Authors
Jegan Sivalingam1, Mathavan Alagarsamy1
Affiliation
Hannah Joseph Hospital, India1,
View Study Report
TCTAP C-030
CORONARY - Acute Coronary Syndromes (STEMI, NSTE-ACS)
Native Vessel or Graft Occlusion- Dilemma of Identifying the Culprit Vessel of Inferior Wall ST Elevation Myocardial Infarction in a Post Coronary Artery Bypass Graft Patient
Jegan Sivalingam1, Mathavan Alagarsamy1
Hannah Joseph Hospital, India1,
Clinical Information
Patient initials or Identifier Number
RR
Relevant Clinical History and Physical Exam
45 years old male with past history of coronary artery bypass graft surgery done six years ago presented with complaints of acute onset chest pain of 6 hours duration. Patient was hemodynamically stable at the time of admission.
Relevant Test Results Prior to Catheterization
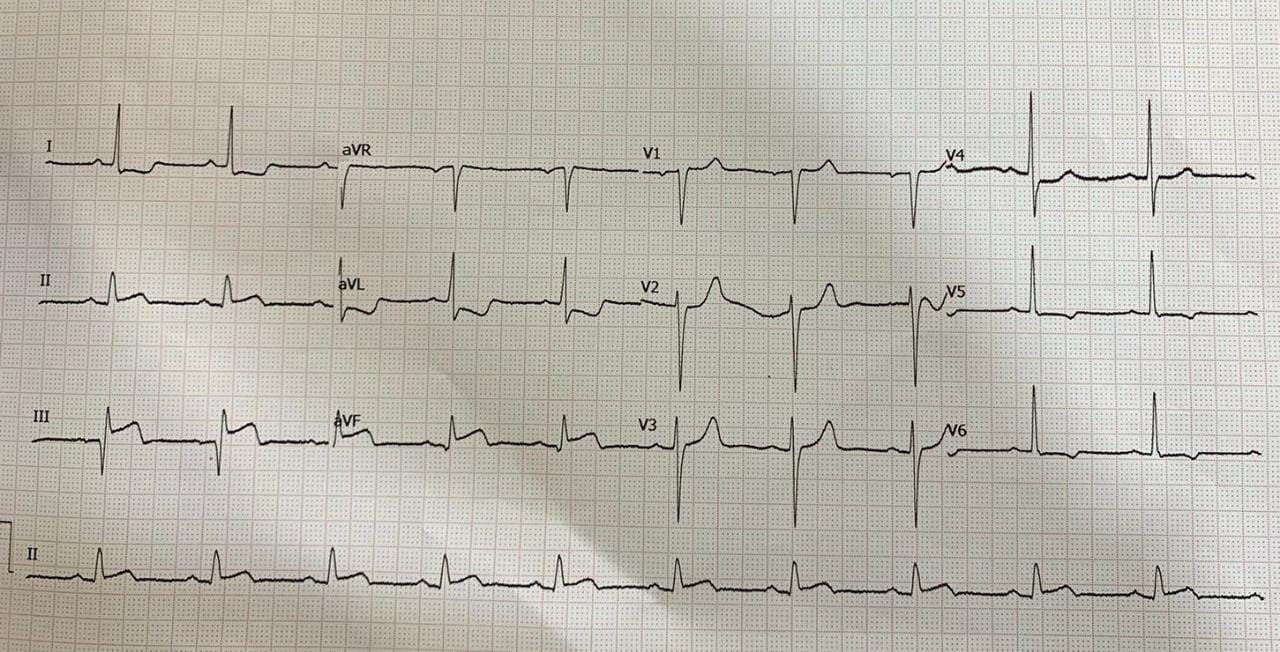
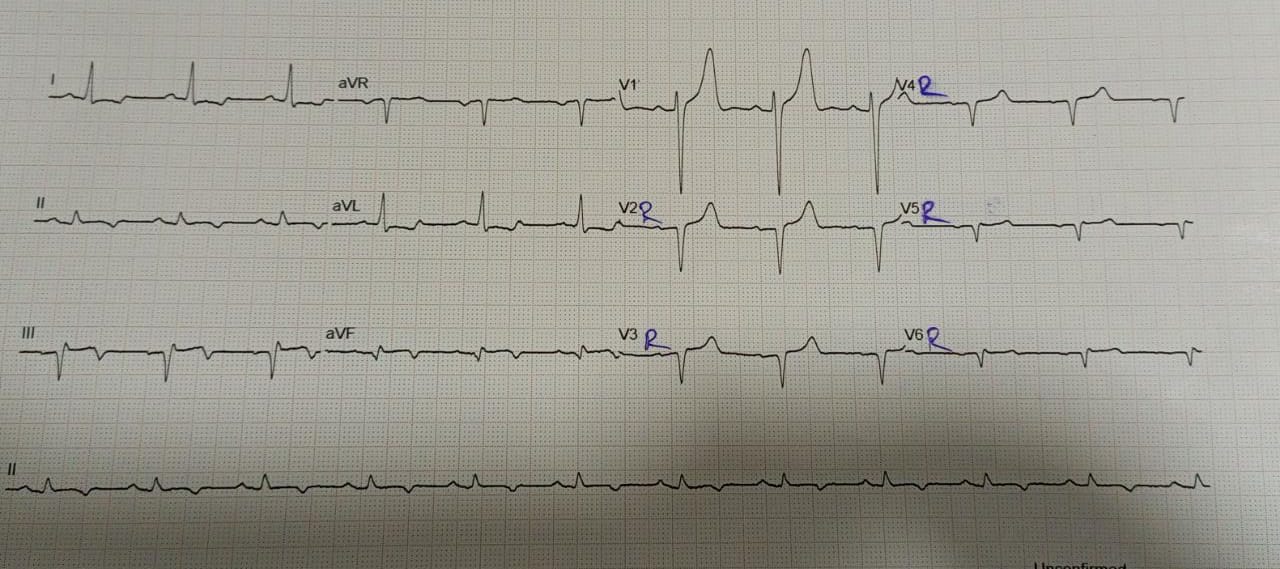
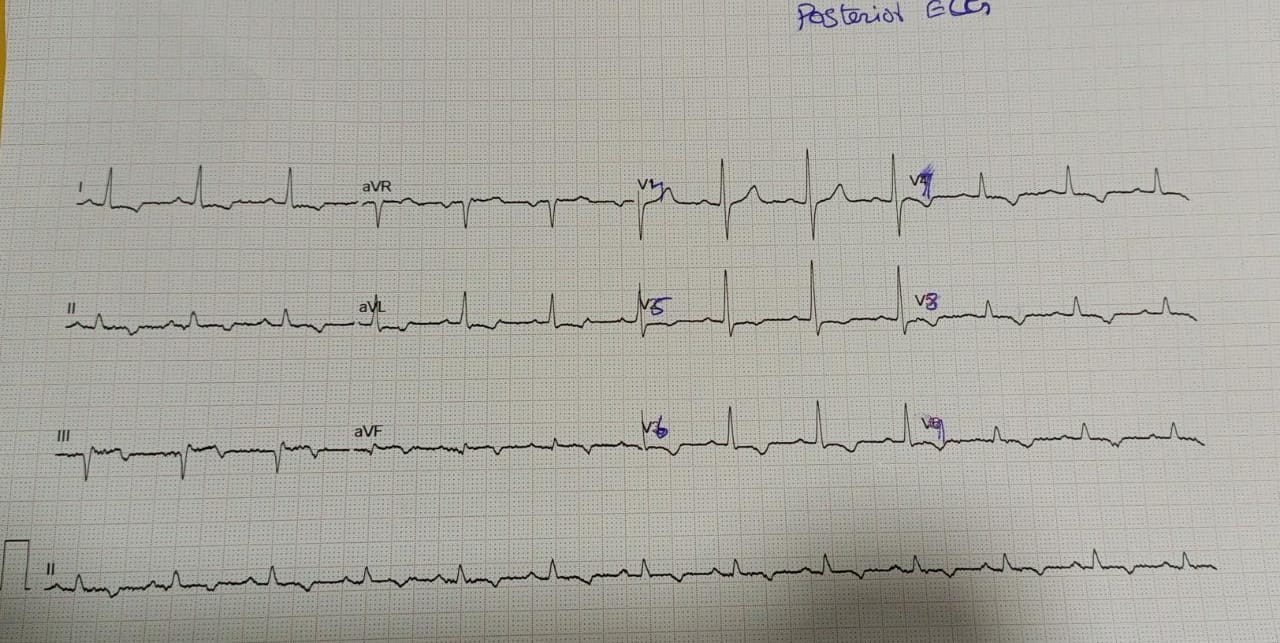
ECG showed Sinus rhythm, ST elevation in II, III, aVF with ST depression in I and aVL suggesting RCA as culprit artery. However, 2D Echocardiogram showed regional wall motion abnormality involving the left circumflex territory, mild left ventricle systolic dysfunction and left ventricular ejection fraction was 43%.
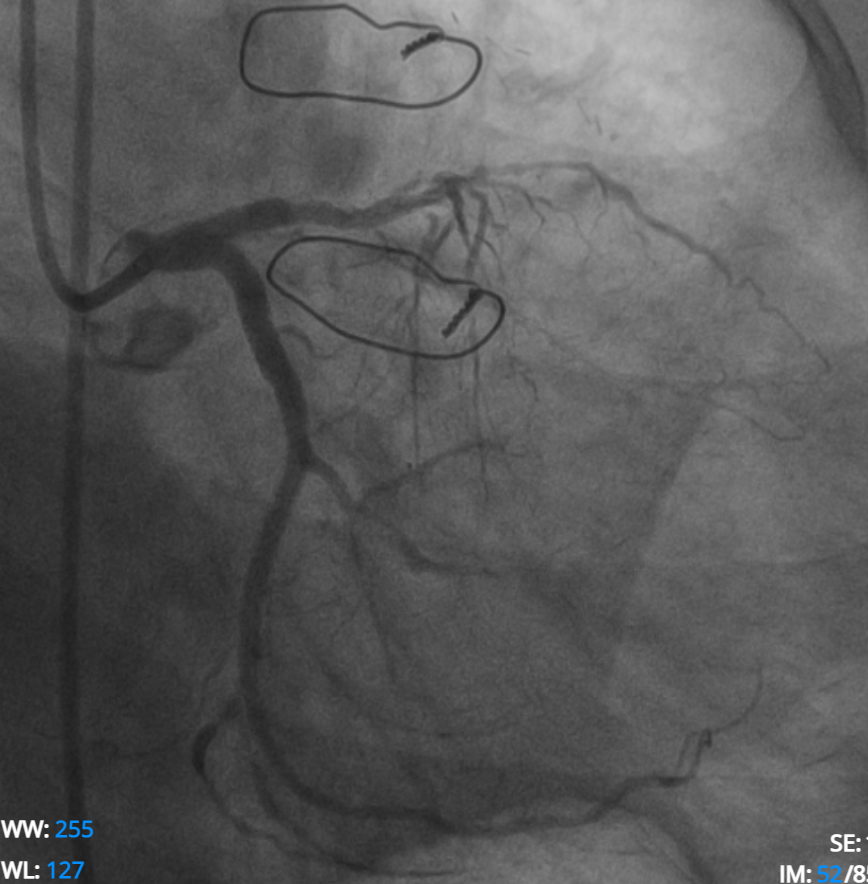
Relevant Catheterization Findings
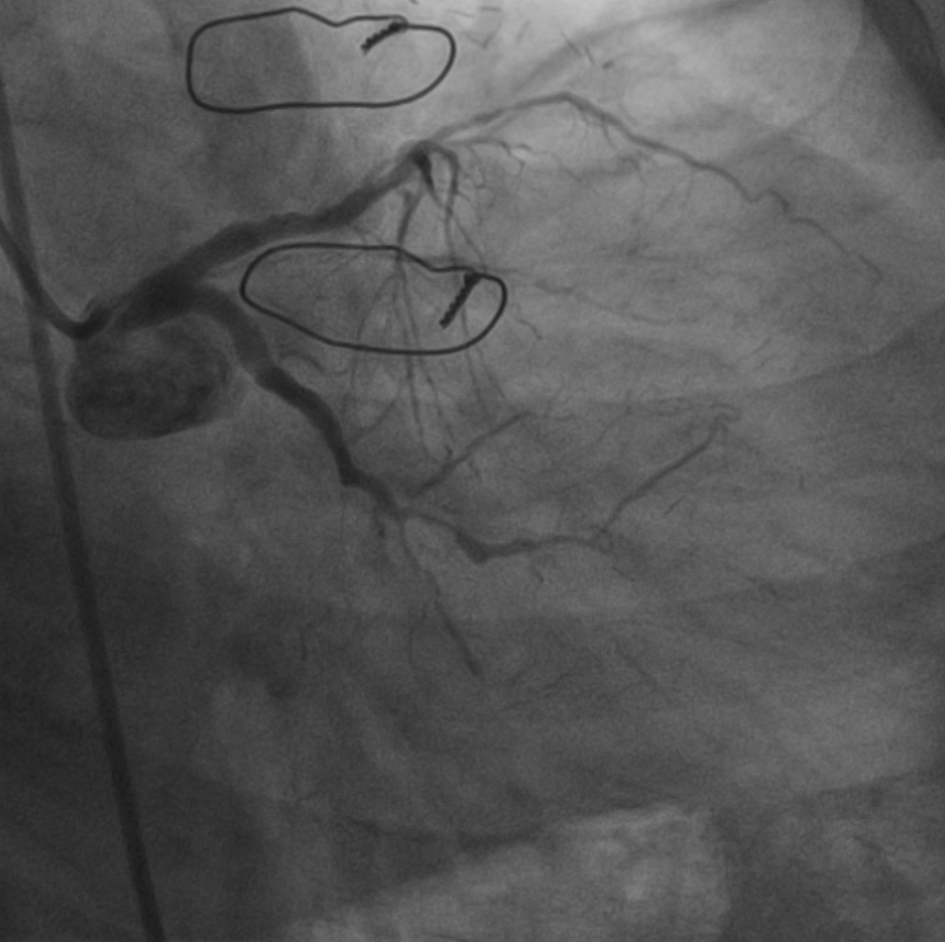
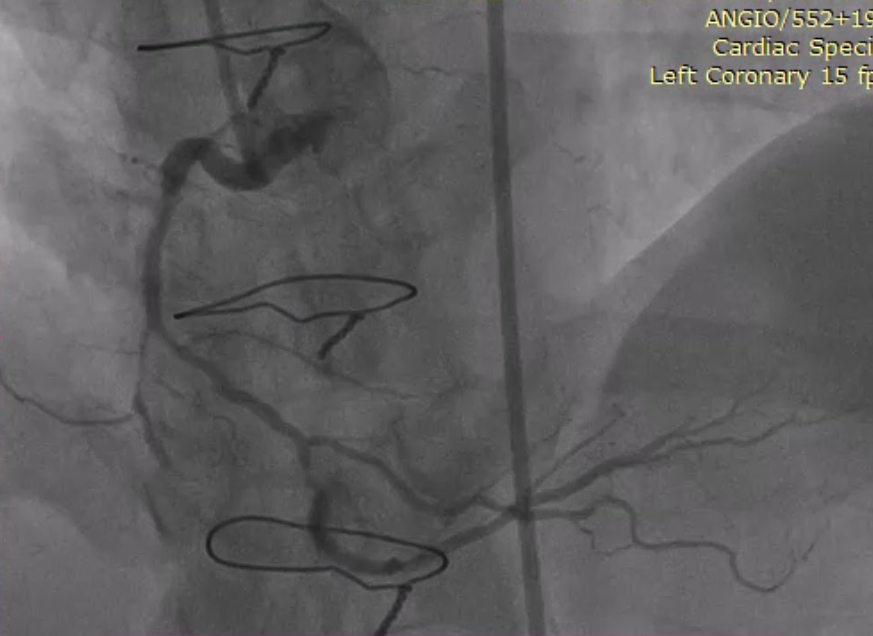
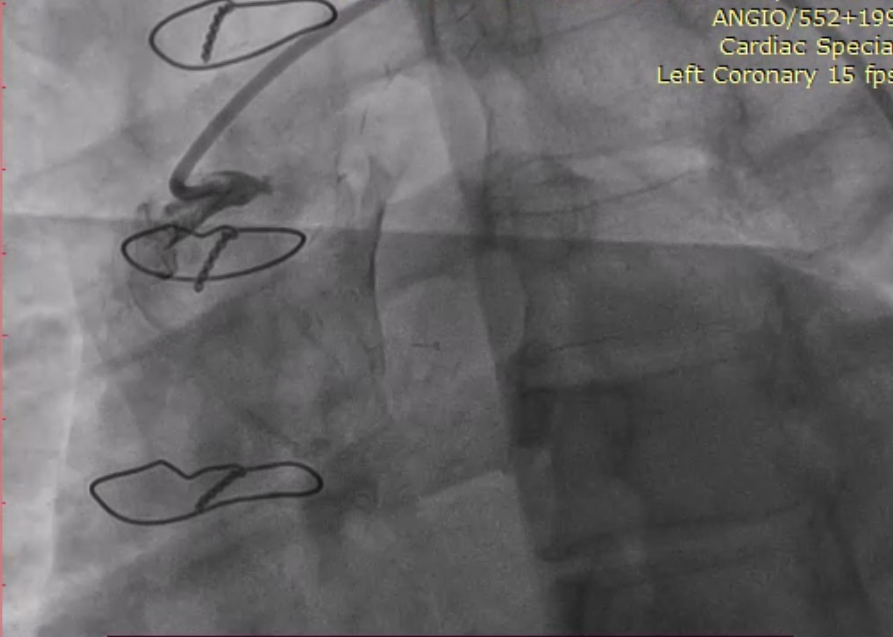
Coronary angiogram showed Native 3 vessel CAD, occluded mid LAD and distal LCX, diffusely diseased RCA, patent LIMA to LAD graft and venous grafts to RCA and OM were occluded. In view of the discordant findings between ECG, Echocardiogram and angiogram, careful review of angiogram revealed that the distal LCX territory was bare and also it correlated with the Echo showing RWMA in inferoposterior wall, so it was identified as the culprit vessel and decided to proceed with PCI of LCX.
Interventional Management
Procedural Step
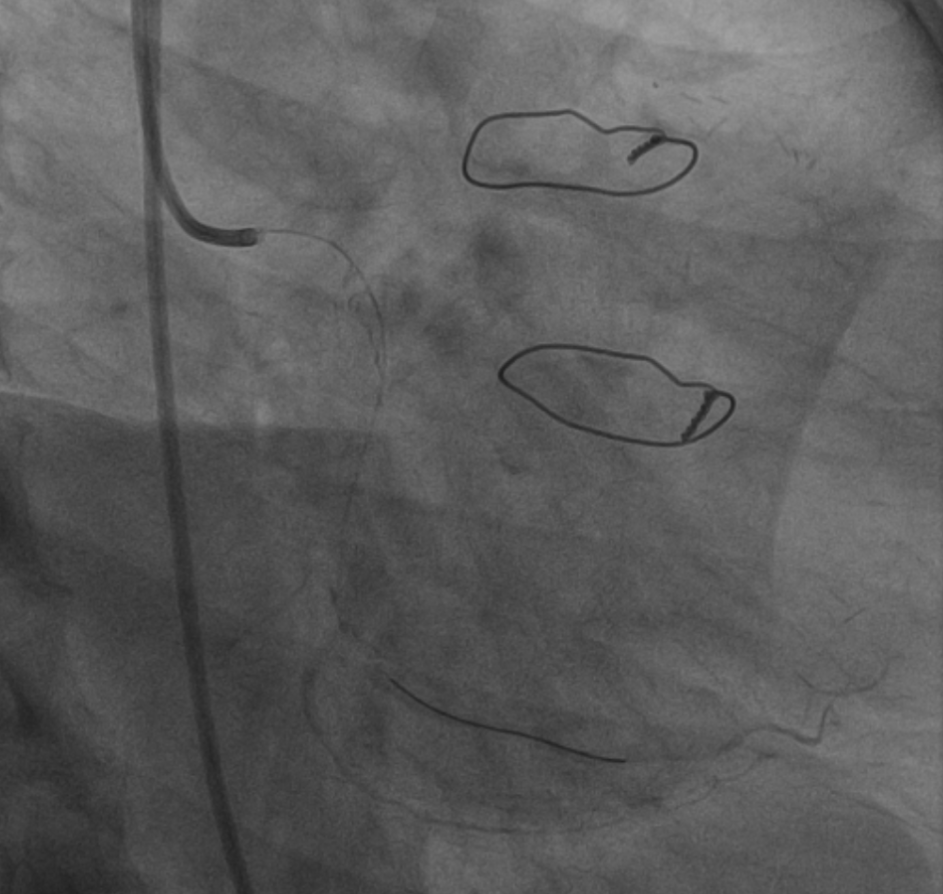
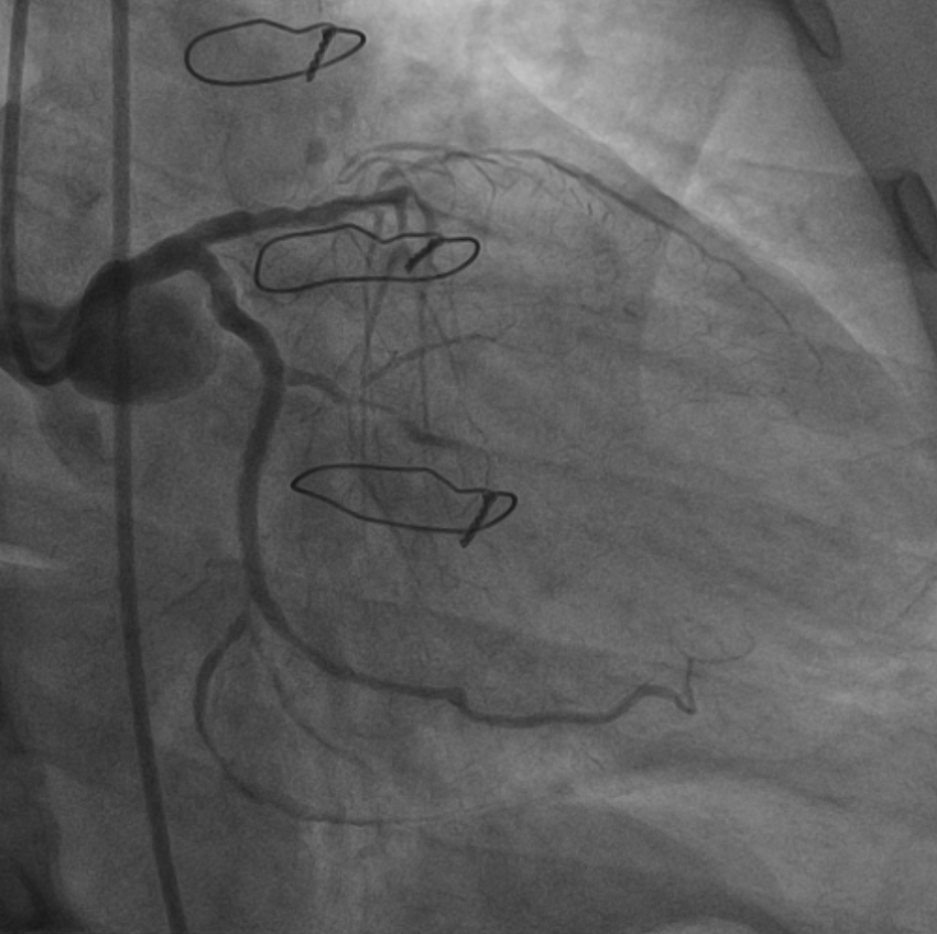
Left circumflex artery was wired with a workhorse coronary guidewire, predilatation done with Artimes 2.0 x 15 mm balloon at 12 atm. The LCX-OM lesion was stented with XIENCE XPEDITION 2.5 x 48 mm stent deployed at 11 atm. Angiogram showed haziness in proximal LCX ? proximal edge dissection with thrombus formation, so it was stented with XIENCE PRIME 3.5 x 18 mm stent deployed at 15 atm overlapping the previous stent. Postdilated with Apollo balloon 3.0 x 10 mm at 18 atm followed by 3.5 x 8 mm Apollo balloon at 18 atm. The final angiogram showed good result, TIMI III flow. There was no dissection/thrombus. Femoral sheath removed in lab and hemostasis achieved by 6F Angioseal.
Case Summary
This case illustrates the dilemma in identifying the culprit artery in a case of inferior wall STEMI in a patient post CABG, non availability of prior angiograms and surgical procedure details was a disadvantage for us. Eventhough we could appreciate a bare area over the distal LCX territory initially we were not sure whether it was a chronic total occlusion or acute occlusion as there was no acute thrombotic stump visible. Finally correlating and corroborating the ECG, Echocardiogram findings and careful review of angiogram led to the identification of the culprit vessel.