
Lots of interesting abstracts and cases were submitted for TCTAP 2023. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-008
Case Report: ST-Elevation Myocardial Infarction in a Patient With Transcatheter Aortic Valve Implantation (TAVI): First Report in Hydra Valve
By Apinya Boonkerng, Anuruck Jeamanukoolkit, Wasant Soonfuang, Sukhum Tachasakunjaroen
Presenter
Apinya Boonkerng
Authors
Apinya Boonkerng1, Anuruck Jeamanukoolkit1, Wasant Soonfuang1, Sukhum Tachasakunjaroen2
Affiliation
Police General Hospital, Thailand1, Ramathibodi Hospital, Thailand2,
View Study Report
TCTAP C-008
CORONARY - Acute Coronary Syndromes (STEMI, NSTE-ACS)
Case Report: ST-Elevation Myocardial Infarction in a Patient With Transcatheter Aortic Valve Implantation (TAVI): First Report in Hydra Valve
Apinya Boonkerng1, Anuruck Jeamanukoolkit1, Wasant Soonfuang1, Sukhum Tachasakunjaroen2
Police General Hospital, Thailand1, Ramathibodi Hospital, Thailand2,
Clinical Information
Patient initials or Identifier Number
P T
Relevant Clinical History and Physical Exam
A 91-year-old man with known symptomatic severe aortic stenosis, underwent TAVI with Hydra valve size 30 mm. replacement in 2018 and presented with acute retrosternal chest pain for 1 hour with dyspnea. At the emergency room, he experienced chest pain with pain score of 6/10. Vital signs showed a BT of 37.2 ℃, BP 164/90 mmHg and PR 140 tpm. Additional medical history included coronary artery disease that had undergone PCI with stenting at LCx and had moderate stenosis at LAD with negative FFR.
Relevant Test Results Prior to Catheterization
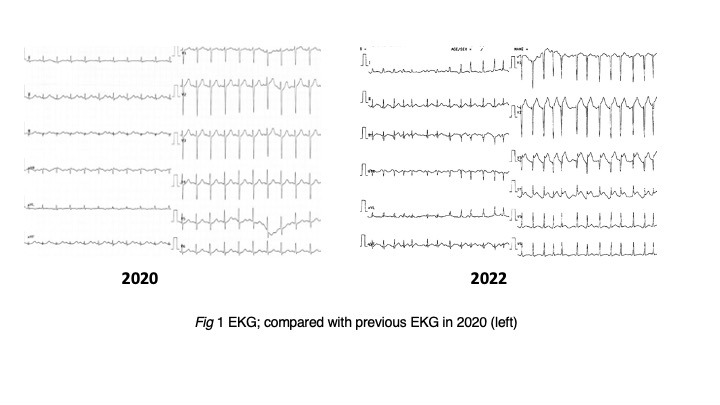
EKG showed AF with rapid ventricular response rate 135 bpm (Fig.1). Chest x-ray showed perihilar congestion, increased cardiomegaly, troponin T 61 ng/L, and NT pro-BNP 1500 pg/ml. An echocardiogram showed mildly reduced LV systolic function (LVEF 45%). Akinesia was observed at the basal to mid-part anterolateral segment and the anteroseptal wall, a well-seated bioprosthetic aortic valve with normal function. He was diagnosed anteroseptal wall ST-elevation ACS with congestive heart failure.
Relevant Catheterization Findings
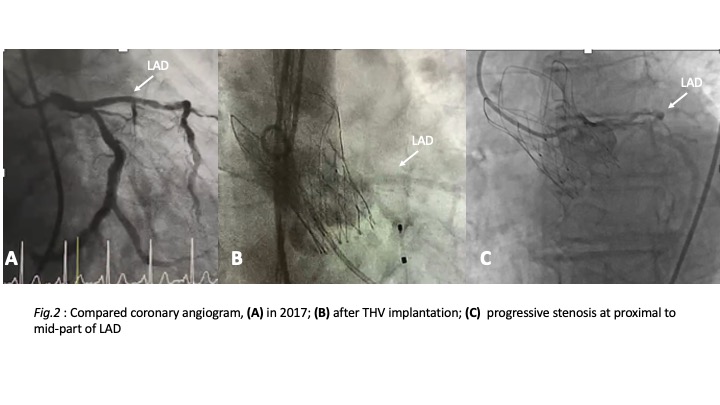
We controlled AF with amiodarone and gave intravenous loop diuretic for congestive heart failure. For respiratory support, we used nasal high flow oxygen. The procedure was performed in the cardiac catheterization laboratory. Right femoral arterial access was obtained then inserted 6 Fr femoral sheath into the right femoral artery. Coronary angiogram showed 90% stenosis at proximal to mid-part of LAD (progressive stenosis compared with previous CAG in 2018) and patent LCx stent (Fig2.).
Interventional Management
Procedural Step
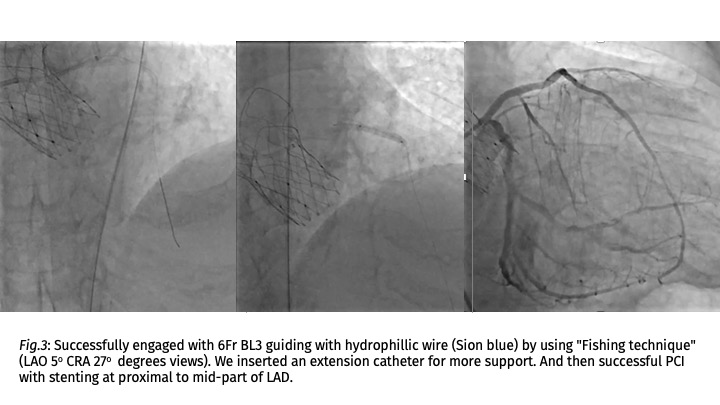
We selected ostial cannulation to the left anterior descending artery (LAD) but found coronary access difficulties. 6Fr JL 3.5 failed to engage coronary ostia then we choose 6Fr XB3 but couldn't engage because of guiding catheter cannot coaxial for coronary ostia. Then we decided to change to engage from the upper frame cell of transcatheter heart valve (THV) because the new-commissure may be obstructed coronary ostia. We successfully engaged with 6Fr BL3 guiding after wiring to left coronary artery with hydrophillic wire (Sion blue) by using "Fishing technique" (LAO 5o CRA 27o degrees views). We inserted an extension catheter for more support. And then successful PCI with stenting at proximal to mid-part of LAD (Fig.3). Total time to balloon 43 mins. No immediate complications. His recovery was uneventful and reported a marked improvement from heart failure. The patient was discharged for the next three days and was clinically stable. We suggest that the first report of ST-elevation acute coronary syndrome from patients with Hydra vale from the Hydra CE registry. Medical records revealed the patient received a Hydra valve size 30 mm. in 2018. The computer tomography for TAVI protocol showed aortic sinus 23.7 mm., aortic sinus 35.6 mm., STJ 27.2 mm., and borderline coronary ostia height (right 11.3 mm., left 11.6 mm.) possible causing coronary access difficulties.
Case Summary
Transcatheter aortic valve implantation (TAVI) has developed rapidly in the past few years and is expected to expand further in the near future. Acute coronary syndrome in patient with TAVI determined an increased risk of death due to longer door-to-wire time and higher PCI failure rate, partial difficulty engaged to coronary ostia, and associated with poor outcome. The additional engagement techniques (changing frame cell of THV, engaged after coronary wiring, using extension guide) were recommended to enhance the success rate of coronary access.