
Lots of interesting abstracts and cases were submitted for TCTAP 2023. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-177
Revascularizing the Re-Stenotic Coronary Artery Following Recanalizing a Chronic Totally Occluded Right Radial Artery via Anatomical Snuffbox
By Hehe Cui, Qingbo Liu, Li Zhou, Hui Chen
Presenter
Hehe Cui
Authors
Hehe Cui1, Qingbo Liu2, Li Zhou2, Hui Chen2
Affiliation
Beijing Anzhen Hospital, Capital Medical University, China1, Beijing Friendship Hospital, China2,
View Study Report
TCTAP C-177
OTHERS - Vascular Access (Transradial)
Revascularizing the Re-Stenotic Coronary Artery Following Recanalizing a Chronic Totally Occluded Right Radial Artery via Anatomical Snuffbox
Hehe Cui1, Qingbo Liu2, Li Zhou2, Hui Chen2
Beijing Anzhen Hospital, Capital Medical University, China1, Beijing Friendship Hospital, China2,
Clinical Information
Patient initials or Identifier Number
WBY/967226
Relevant Clinical History and Physical Exam
A 69-year-old male smoker complaint frequent transient rest chest tightness within 2 days. The symptom radiated to the jaw and lasted almost 20 minutes. He had a poorly controlled hyperlipidemia for 3 years, a coronary stenting history [ left anterior descending artery (LAD) and the first diagonal artery (D1) ] for 1.5 years, and he underwent lower extremity angioplasty one year before. Physical examination found the right radial pulse was impalpable while the left pulse was normal.
Relevant Test Results Prior to Catheterization
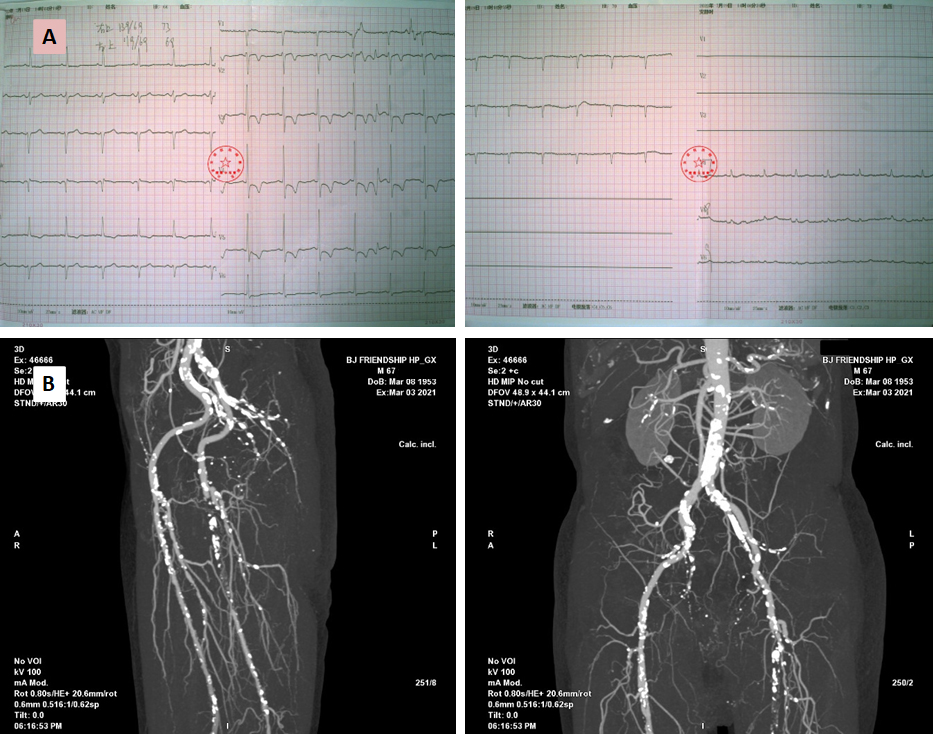
An EKG was acquired (Figure 1A). Cardiac troponin I 0.076 ng/mL (99 % URL 0.030). LDL-C 2.25 mmol/L. Echocardiogram showed reduced ejection fraction (48 %) and hypokinetic anterior wall motion. The computed tomographic angiography of the lower extremities one year before showed stenosis and calcified plaques involving bilateral iliac and left popliteal arteries (Figure 1B). The patient was diagnosed with non-ST elevation myocardial infarction.
Relevant Catheterization Findings
The right distal radial artery (dRA) was punctured successfully via the anatomical snuffbox. Although a good blood flow from the puncture needle soft sheath was demonstrated, a Sion guidewire failed to advance. Thus, we performed a radial angiography through the needle sheath which showed total occlusion of the right radial artery and a good collateral circulation from the ulnar artery (Video Figure 1).

Interventional Management
Procedural Step
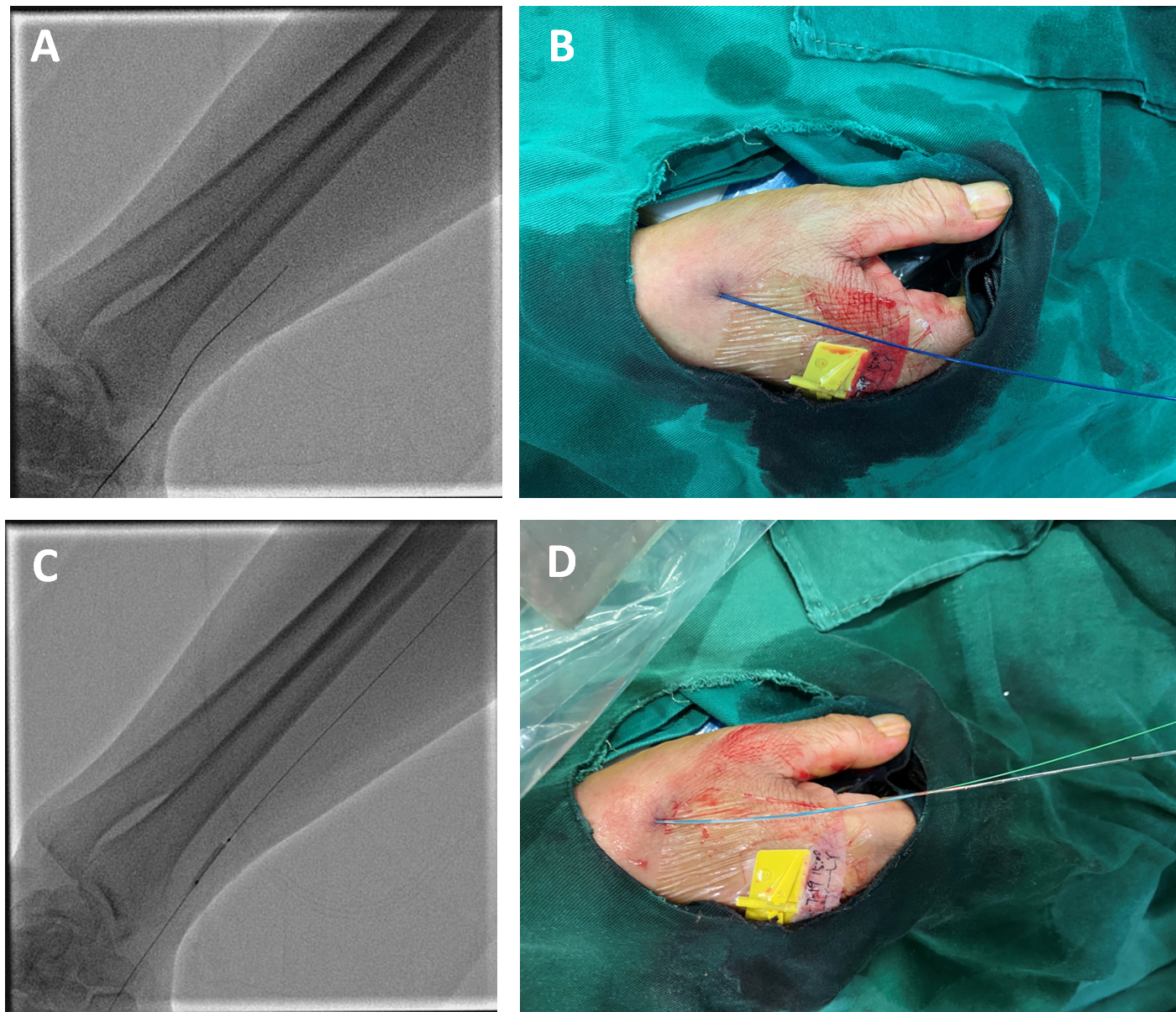
With support of a 1.9F microcatheter (MC), a Fielder XT-A guidewire passed through the occlusion and the MC was advanced along (Figure 2A and B). Tip injection from MC confirmed the intralumenal course, and the Sion was switched back as a workhorse. The occlusion was pre-dilated with a balloon (2.0 mm × 15 mm) at 10 - 12 atmospheric pressure (Figure 2C and D), and a 6F radial sheath was inserted.
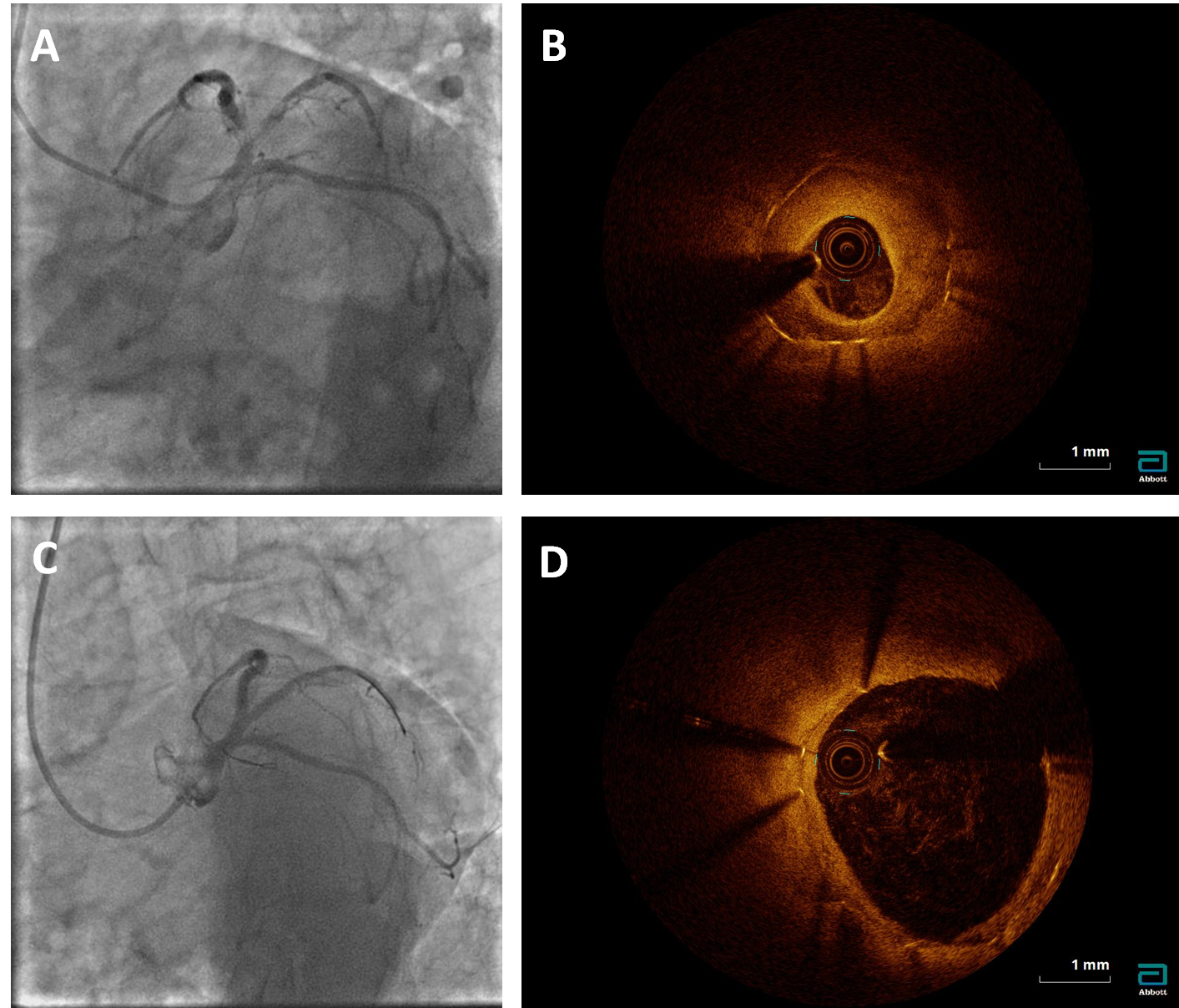
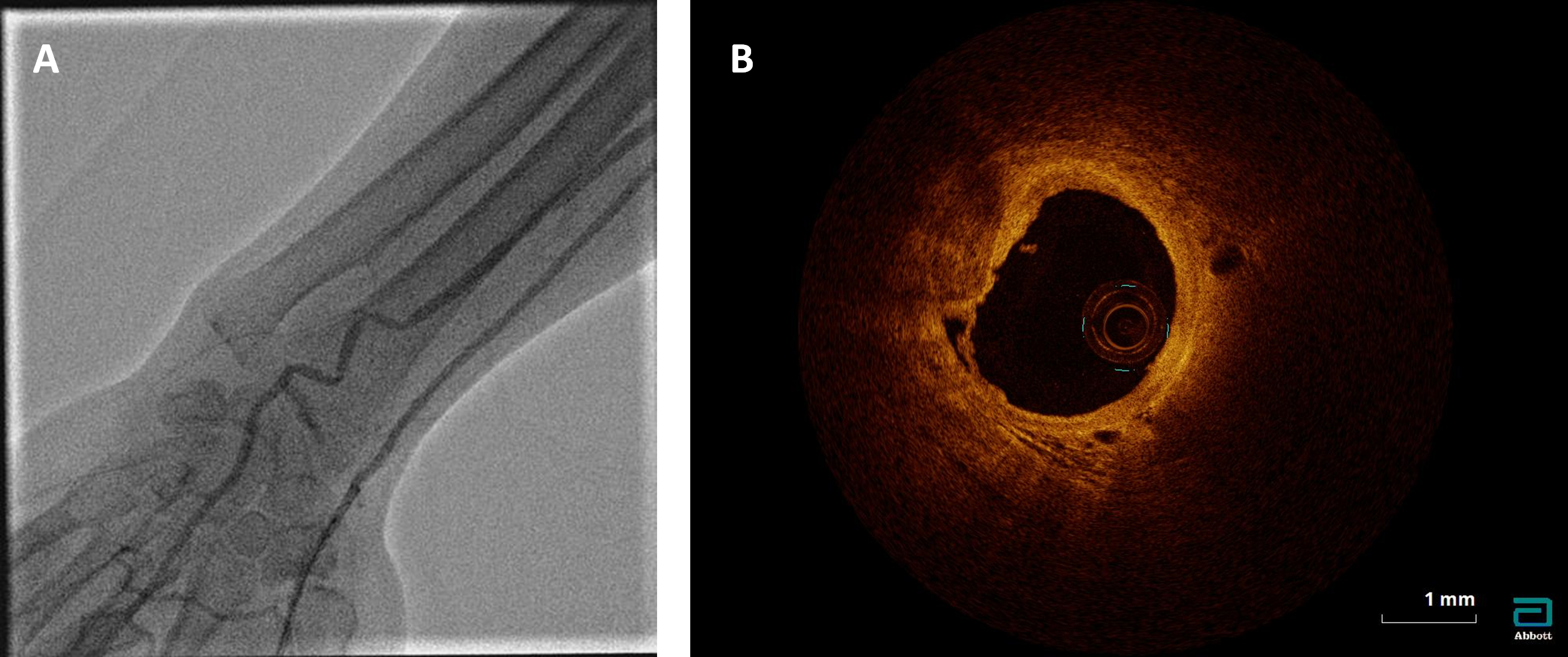
The coronary angiography using 5F Tig catheter showed almost 99 % restenosis at the bifurcation of the proximal stented LAD and D1 (Figure 3A). A 6F LeftBU 3.25 guiding catheter was cannulized. A Marvel guidewire and the Sion were separately advanced to the distal LAD and D1. After pre-dilation with a 1.5 mm × 15 mm balloon, an optical coherence tomography (OCT) analysis was performed which found a homogeneous intrastent plaque in the LAD (Figure 3B). Thus, the lesions in D1 and LAD were sequentially and adequately pre-dilated, and a 2.75 mm × 30 mm drug-coated balloon (DCB) was used in D1 and a 3.5 mm× 20 mm DCB was used in LAD. OCT showed a residual stenosis less than 10% (Figure 3C and D). After removing the catheter and the sheath, radial angiography showed a resumed radial blood flow, and the OCT imaging found a patent arterial lumen, as well as a calcified plaque in the previous punctured site (Figure 4A and B).
Case Summary
The radial artery occlusion is a common complication of the routine transradial access for coronary angiography and intervention. Distal radial artery (dRA) access is a novel approach with great advantage of reducing radial arterial occlusive rate and improving patient comfort of post-operative bandaging. More importantly, recanalizing the totally occluded radial artery via anatomical snuffbox is a unique advantage of dRA access, which resumed the radial blood flow and avoided puncture injury to other arteries. In this case, post-operative OCT imaging explored that the calcified plaque formation at previously punctured site might be one of the reasons for radial occlusion.