
Lots of interesting abstracts and cases were submitted for TCTAP 2023. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-004
Kill Two Birds With One Stone: Primary Coronary Intervention for Acute Total Occlusion Left Anterior Descending and Right Coronary Arteries in ST-Segment Elevation Myocardial Infarction
By Ayman Azoz
Presenter
Ayman Azoz
Authors
Ayman Azoz1
Affiliation
Armed Forces Hospitals Southern Region, Saudi Arabia1,
View Study Report
TCTAP C-004
CORONARY - Acute Coronary Syndromes (STEMI, NSTE-ACS)
Kill Two Birds With One Stone: Primary Coronary Intervention for Acute Total Occlusion Left Anterior Descending and Right Coronary Arteries in ST-Segment Elevation Myocardial Infarction
Ayman Azoz1
Armed Forces Hospitals Southern Region, Saudi Arabia1,
Clinical Information
Patient initials or Identifier Number
SH3501085555
Relevant Clinical History and Physical Exam
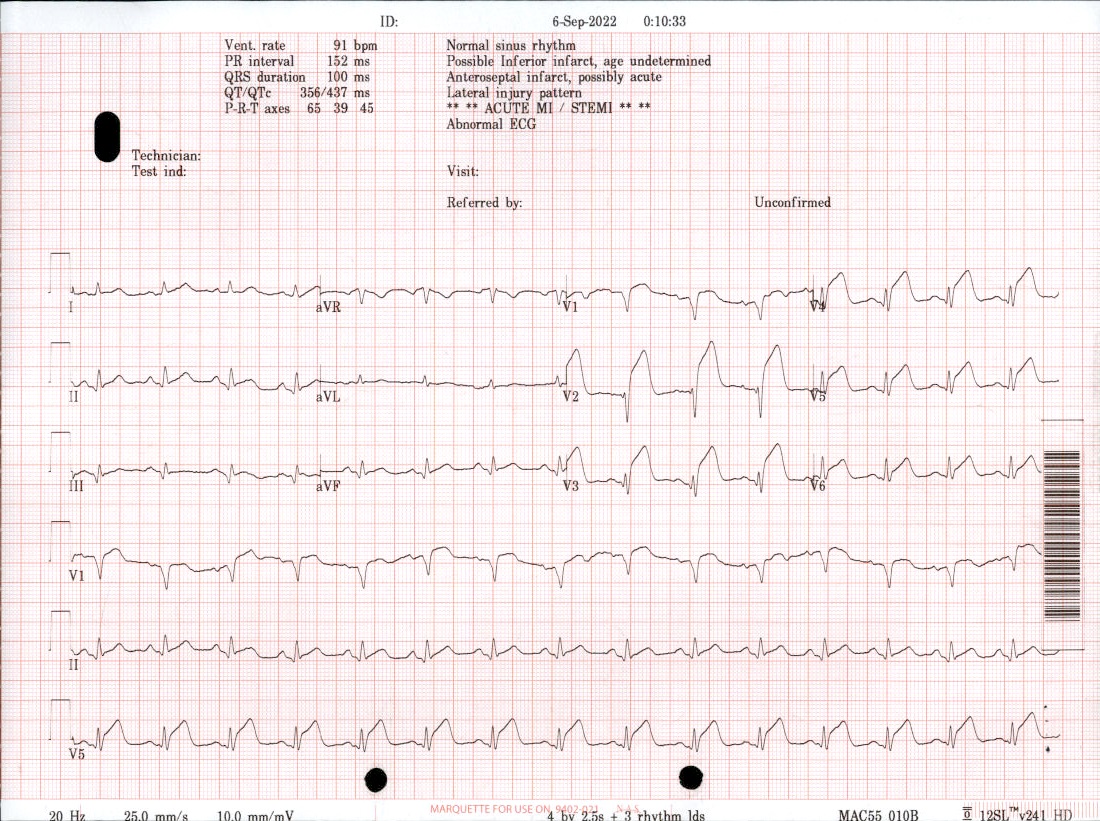
55 year Saudi old male patient; hypertensive; diabetic and heavy smoker presented to us with typical chest pain that started 2 hours before presentation in ER. ECG done showed ST segment elevation in V1 - V6 and a slight elevation in leads II; III and Avf. Cardiac enzymes were elevated. Cath lab was activated and the patient was transferred directly to the cath lab.
Relevant Test Results Prior to Catheterization
hs-cTni 1050 ng/mL then became 8700 ng/mLSerum Creatinine 67 µmol/L
Relevant Catheterization Findings
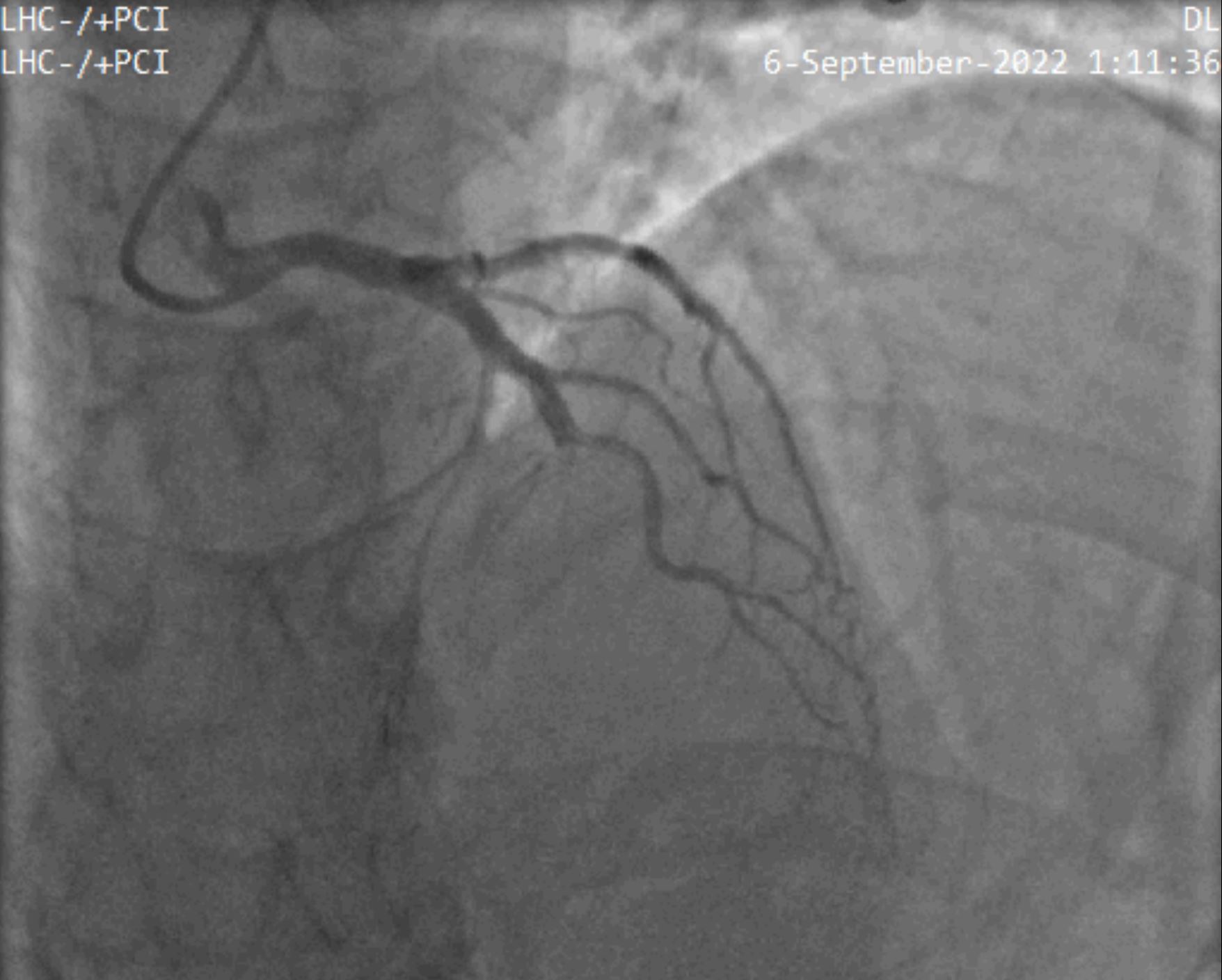
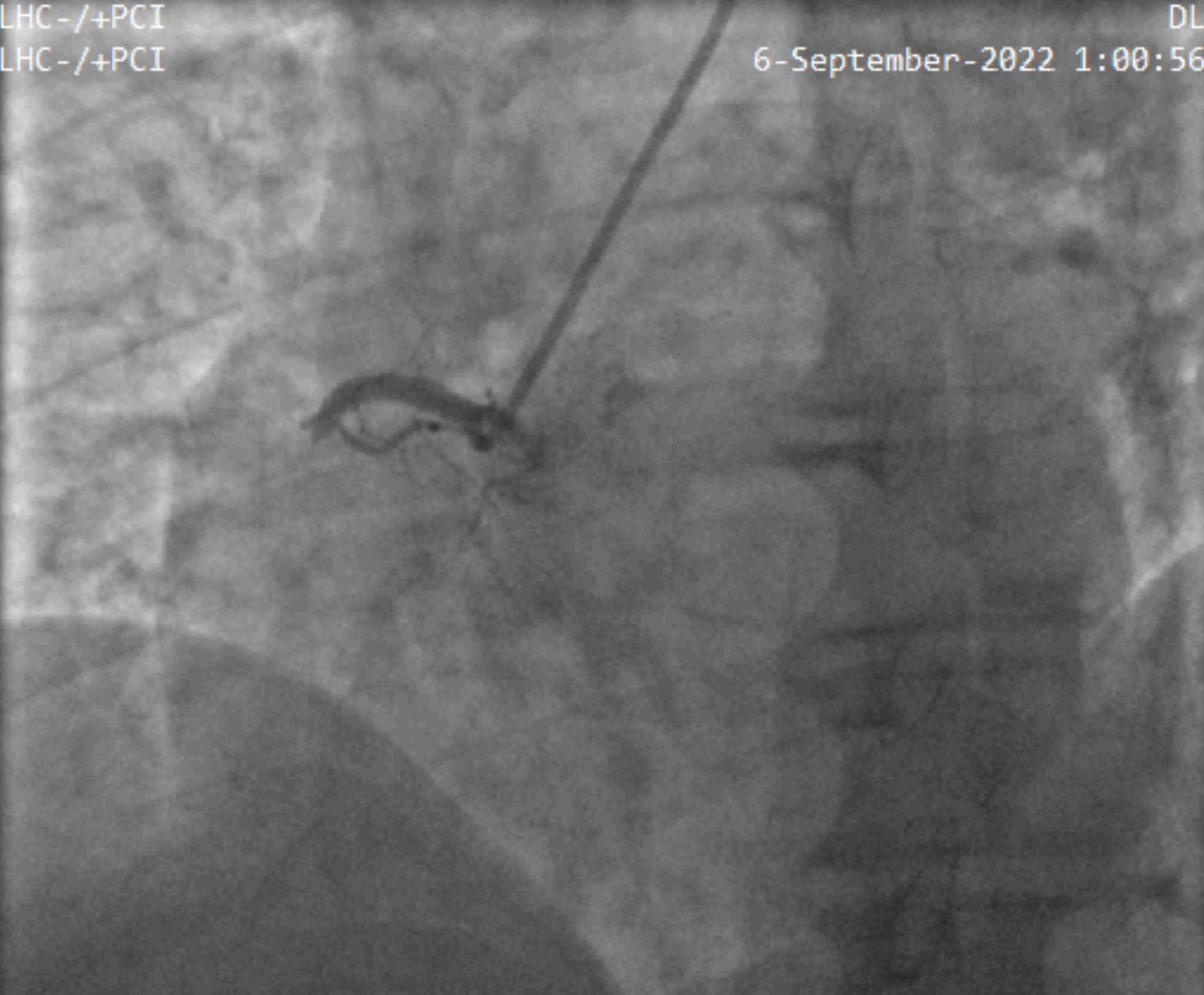
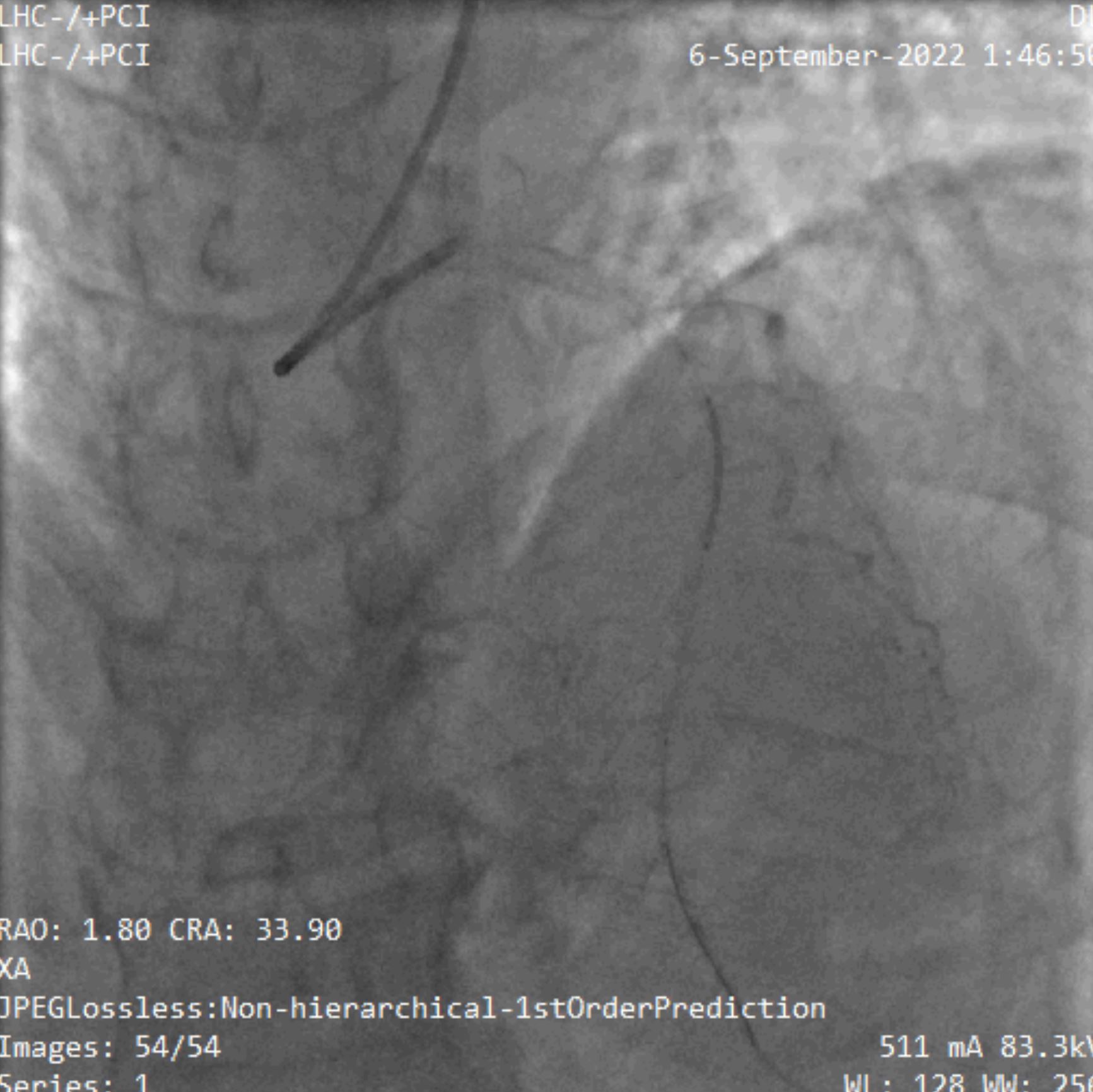
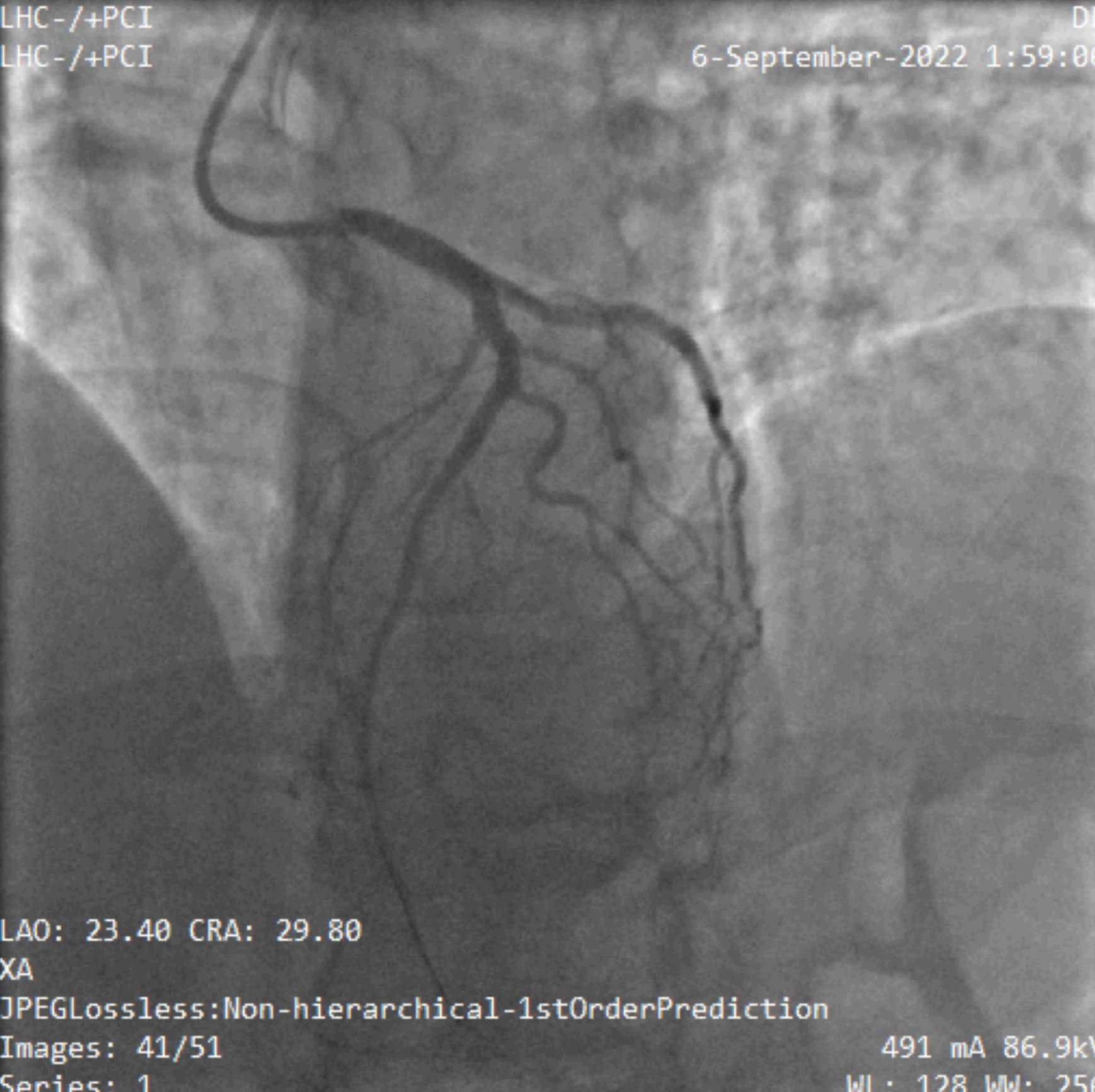
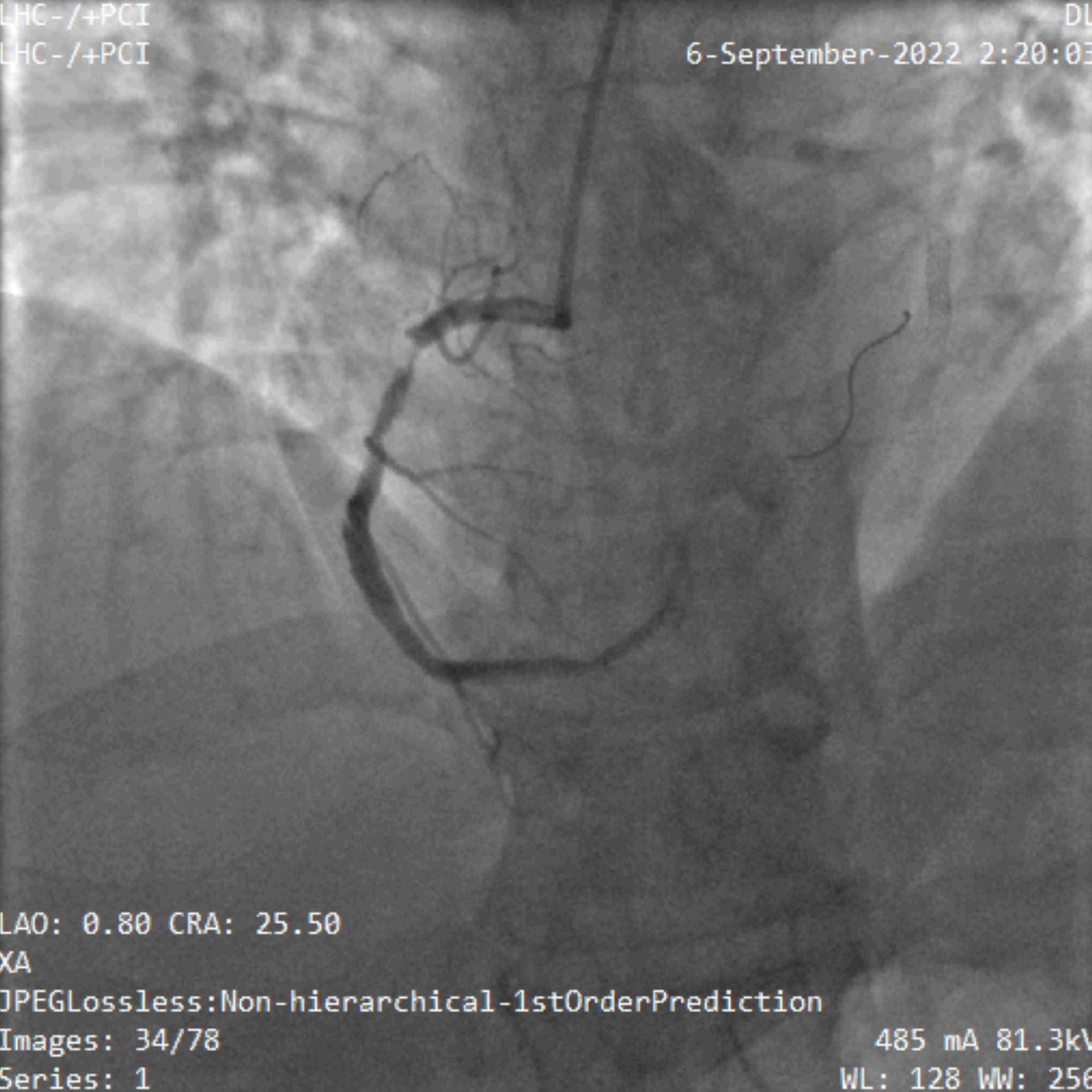
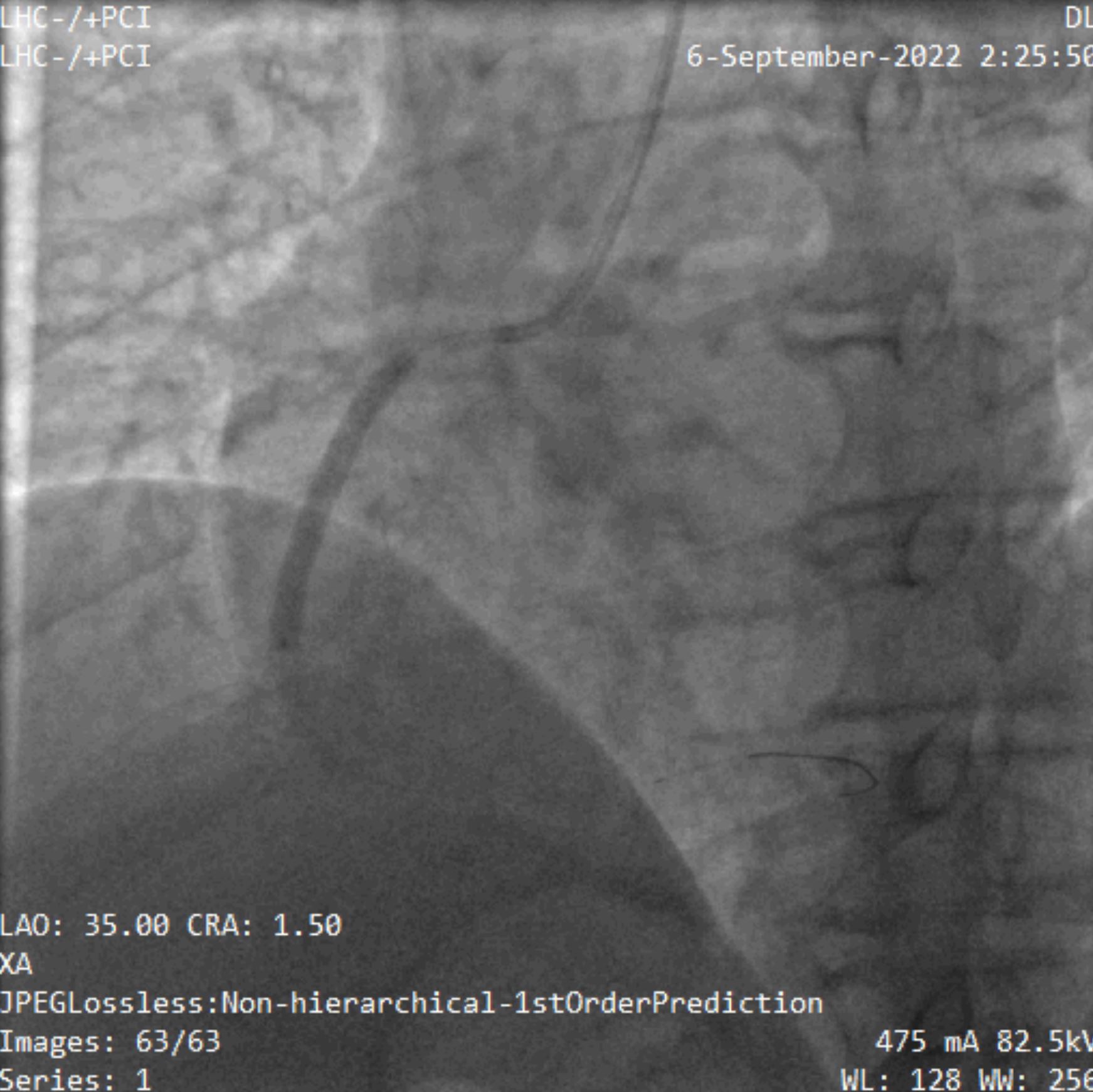
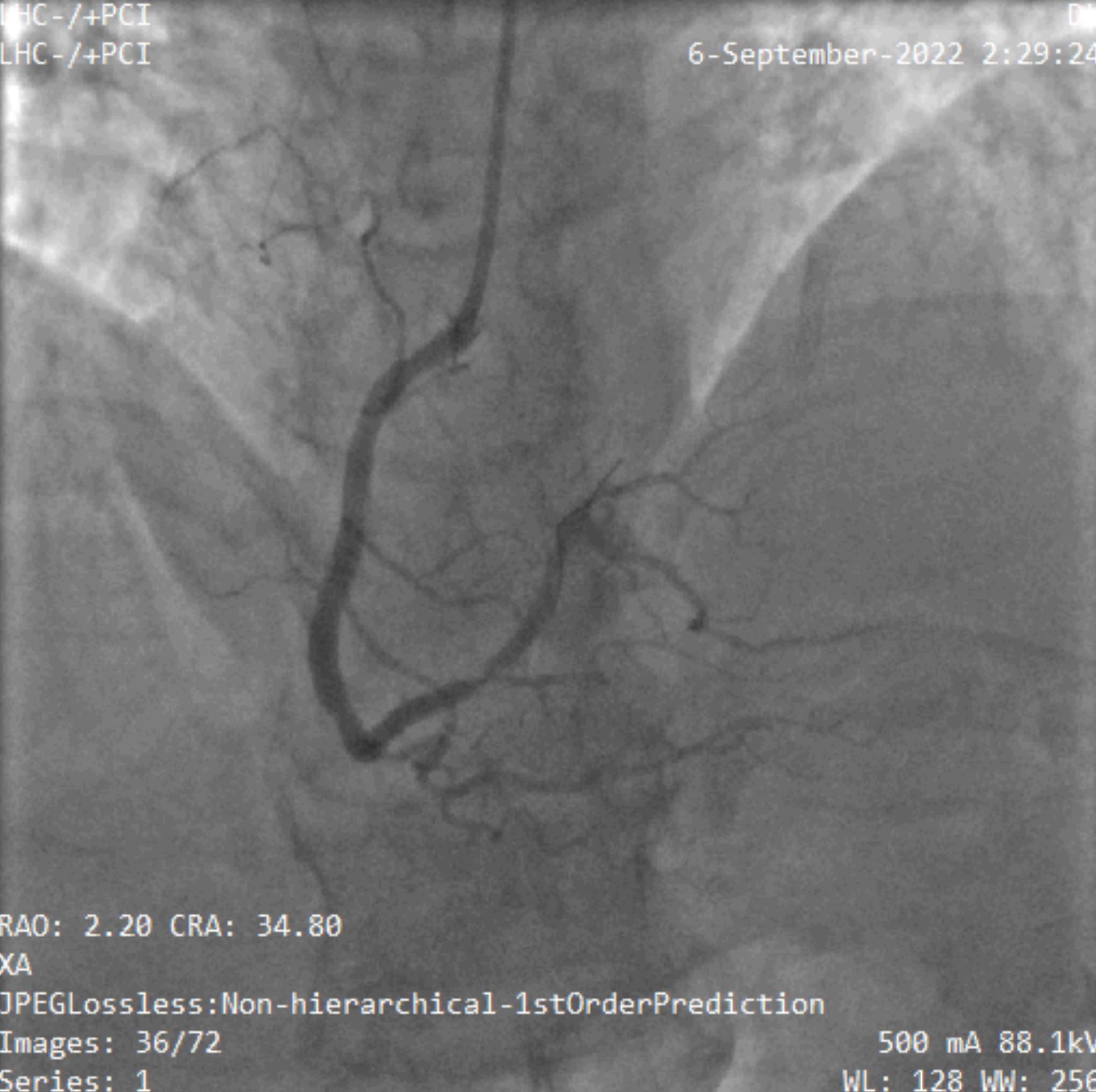
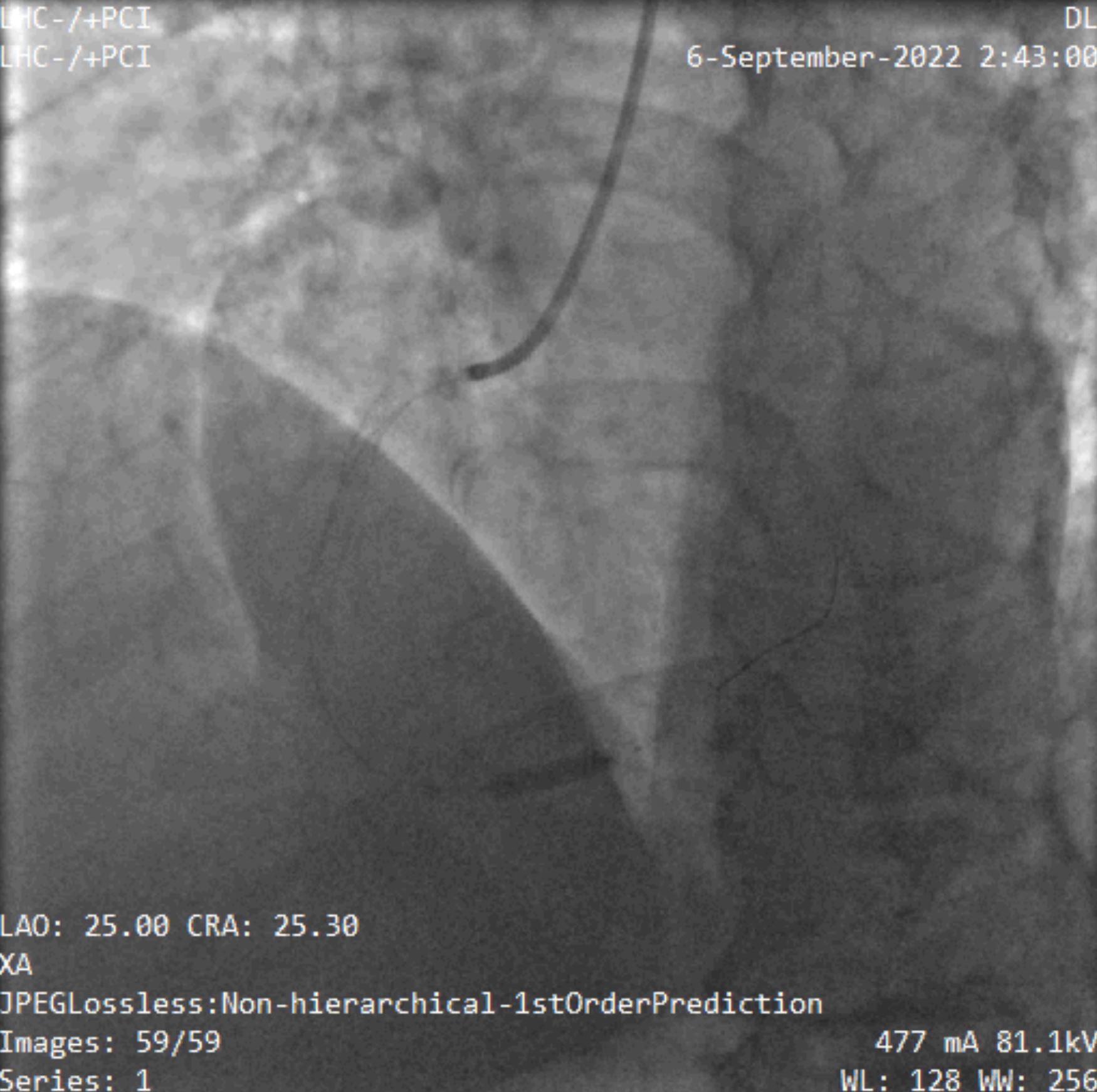
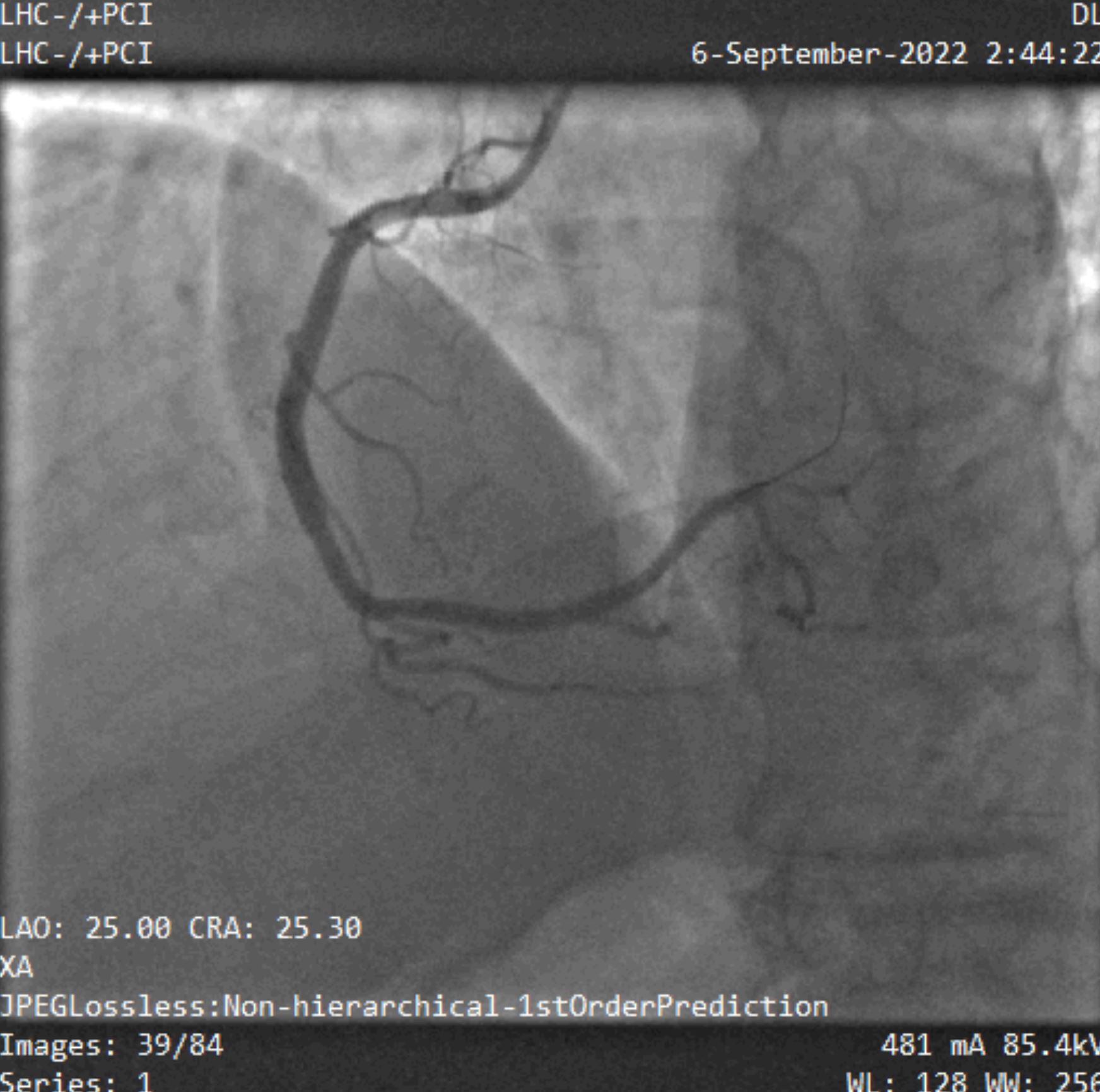
Through Rt Radial ApproachLM: Atherosclerotic artery that bifurcates to LAD and LCX; no significant lesionLAD: Atherosclerotic long artery; had mild irregularities that wrap around the apex and had 3 diagonals and multiple septal perforators. LAD was acutely totally occluded from its mid-segment after the 3rd diagonal.LCX: Non-dominant vessel; had mild luminal irregularities; no significant stenosisRCA: Atherosclerotic Dominant vessel; acute totally occluded from its proximal segment.
Interventional Management
Procedural Step
Guiding Catheter: LCA: EBU 3.5 6 Fr. RCA: JR 4.0 6 Fr.PCI to LAD : The LM was engaged by EBU 3.5 6 Fr. Guiding catheter; a 0.014’’ BMW wire was advanced to the distal LAD with the assistance of Sprinter Legend balloon 2.25 x 15 mm then inflated at the lesion site multiple times up to 18 ATM. A DES Resolute Onyx 3.0 X 22 mm was adjusted at the lesion site and deployed at 12 ATM. Slow flow of the LAD was noted NTG and Nitroprusside injected intracoronary then TIMI III flow achieved and no instant complication.
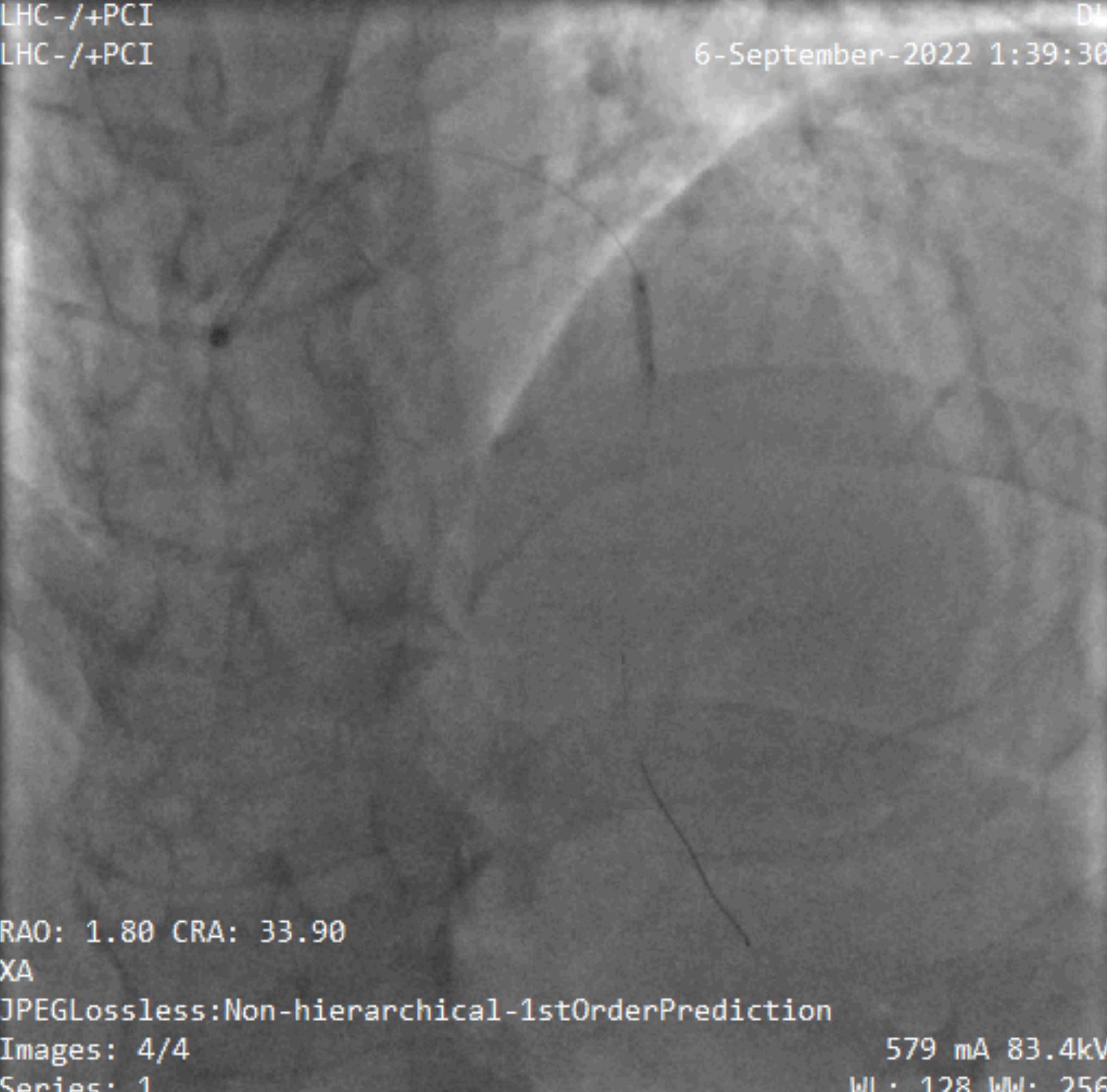
PCI to RCA: The RCA was engaged by JR 4.0 Guiding catheter; a 0.014’’ BMW wire was advanced to distal RCA. A Sprinter Legend balloon 2.0 x 20 mm then inflated at the lesion site multiple times up to 18 ATM. A DES Resolute Onyx 4.0 X 38 mm was adjusted at the lesion site and deployed at 12 ATM. After achieving good distal flow we noticed distal RCA had focal 70% stenosis (after giving NTG) So; A DES Resolute Onyx 3.0 X 12 mm was adjusted at the lesion site and deployed at 12 ATM. TIMI III flow was achieved and no instant complication.
PCI to RCA: The RCA was engaged by JR 4.0 Guiding catheter; a 0.014’’ BMW wire was advanced to distal RCA. A Sprinter Legend balloon 2.0 x 20 mm then inflated at the lesion site multiple times up to 18 ATM. A DES Resolute Onyx 4.0 X 38 mm was adjusted at the lesion site and deployed at 12 ATM. After achieving good distal flow we noticed distal RCA had focal 70% stenosis (after giving NTG) So; A DES Resolute Onyx 3.0 X 12 mm was adjusted at the lesion site and deployed at 12 ATM. TIMI III flow was achieved and no instant complication.
Case Summary
Simultaneous coronary thrombus and acute occlusion in multiple coronary arteries are incredibly rare and have higher mortality rates.