
Lots of interesting abstracts and cases were submitted for TCTAP 2023. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-137
Left Main Angioplasty in a Complex Patient on ECMO Support
By Amitabh Yaduvanshi, Vikas Kataria, Mohit M Bhagwati, Ishita Yaduvanshi
Presenter
Amitabh Yaduvanshi
Authors
Amitabh Yaduvanshi1, Vikas Kataria1, Mohit M Bhagwati1, Ishita Yaduvanshi2
Affiliation
Holy Family Hospital, India1, Baba Saheb Ambedkar Medical College and Hospital, India2,
View Study Report
TCTAP C-137
CORONARY - Hemodynamic Support and Cardiogenic Shock
Left Main Angioplasty in a Complex Patient on ECMO Support
Amitabh Yaduvanshi1, Vikas Kataria1, Mohit M Bhagwati1, Ishita Yaduvanshi2
Holy Family Hospital, India1, Baba Saheb Ambedkar Medical College and Hospital, India2,
Clinical Information
Patient initials or Identifier Number
M M
Relevant Clinical History and Physical Exam
63-year-old male, known diabetic for the last 8 years, on and off treatment, presented with retrosternal burning for the last 3 days and severe breathlessness and sweating for the last 4 hours.
Relevant Test Results Prior to Catheterization
ECG showed LBBBEcho: global LV dysfunction with EF of 30%, moderate MR
Relevant Catheterization Findings
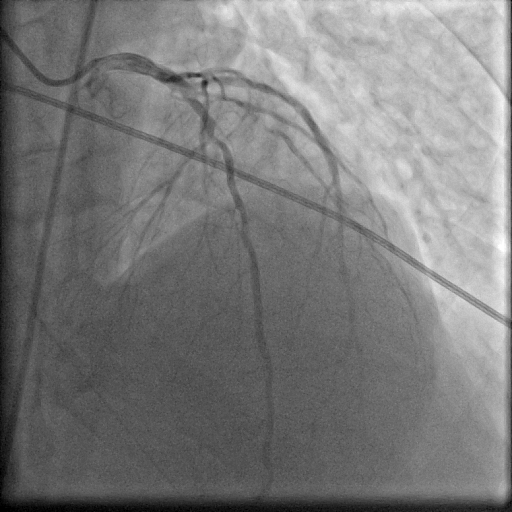
A coronary Angiogram showed significant disease at the Left Main ostium and Proximal LAD. [Figure A, Figure B] the left circumflex had proximal plaquing. the RCA showed diffuse plaquing with significant stenosis in the PLB.

Interventional Management
Procedural Step
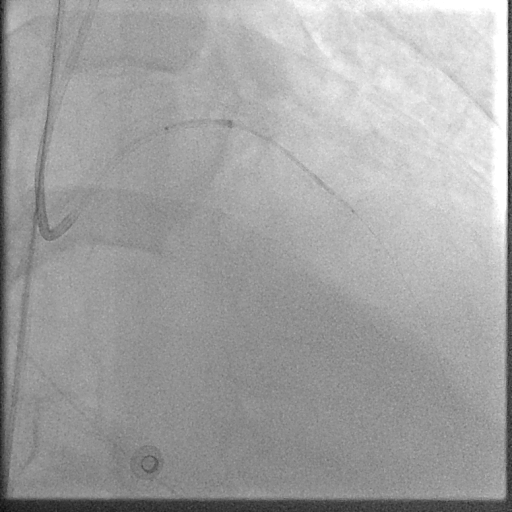
The patient was put on ECMO support and advised CABG. A surgical opinion was taken and high surgical risk was explained to the attendants who did not give consent for surgery. After 5 days on ECMO, the attendants agreed to high-risk angioplasty of LM and LAD.Since the patient had IABP in the right femoral artery, the ECMO return cannula in the left femoral artery was used for arterial access and the tubing was punctured with 6F sheath. [Figure 3]The LM was engaged with 6 F guiding catheter, the LAD lesion was pre-dilated with NC balloon, and a 3.5 X 48 mm stent was deployed from distal to proximal LAD with the help of a Guide Extension Catheter [Figure 4]. A 4.0 X 18 mm stent was then deployed from the LM ostium to LAD and POT was done with a 4.5 mm NC balloon, there was no significant compromise of the LCx ostium [Figure 5]. A dissection at the distal edge of the LAD stent was covered with a 3.0 x 15 mm stent deployed with the help of a guide extension catheter. At the end of the procedure, the ECMO tubing at the site of sheath insertion was cut and the tube was reattached to the return cannula.IABP was removed on 2nd post-procedure day.


Case Summary
Patients who present with stage D or E cardiogenic shock require prompt mechanical cardiac support before attempting revascularisation.