
Lots of interesting abstracts and cases were submitted for TCTAP 2023. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-042
A Case of Successful Thrombus Aspiration in a Patient With Intermediate-High Risk Pulmonary Embolism
By An Shing Ang, Randal Jun Bang Low, Fahim Jafary
Presenter
An Shing Ang
Authors
An Shing Ang1, Randal Jun Bang Low1, Fahim Jafary1
Affiliation
Tan Tock Seng Hospital, Singapore1,
View Study Report
TCTAP C-042
CORONARY - Adjunctive Procedures (Thrombectomy, Atherectomy, Special Balloons)
A Case of Successful Thrombus Aspiration in a Patient With Intermediate-High Risk Pulmonary Embolism
An Shing Ang1, Randal Jun Bang Low1, Fahim Jafary1
Tan Tock Seng Hospital, Singapore1,
Clinical Information
Patient initials or Identifier Number
LLY
Relevant Clinical History and Physical Exam
A 46 year old lady with no past history was admitted for left MCA infarct. She was also diagnosed with ovarian cancer. She then complained of painful unilateral left lower limb swelling with non-pitting edema, before subsequently developing tachycardia and hypoxemic respiratory failure.
Relevant Test Results Prior to Catheterization
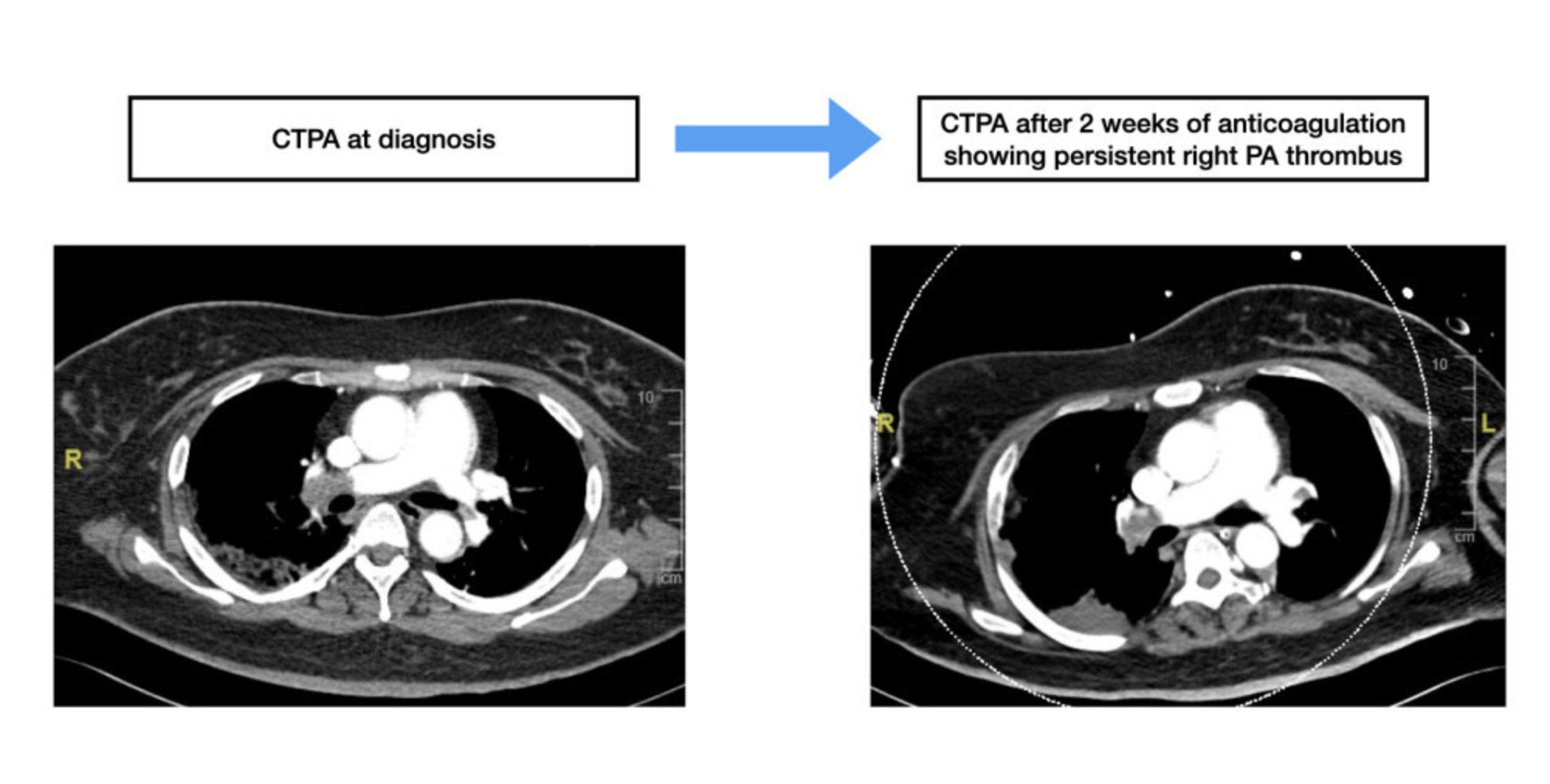
Computed tomography pulmonary angiogram (CTPA) showed bilateral pulmonary embolism. Despite 2 weeks of the therapeutic anticoagulation, she became increasingly tachycardic with rapidly increasing oxygen requirements, up to high flow nasal oxygen therapy. A repeat CTPA (Figure A) showed persistent extensive right sided PE, with right heart strain. Echocardiography revealed a dilated right ventricle with flattened interventricular septum.
Relevant Catheterization Findings
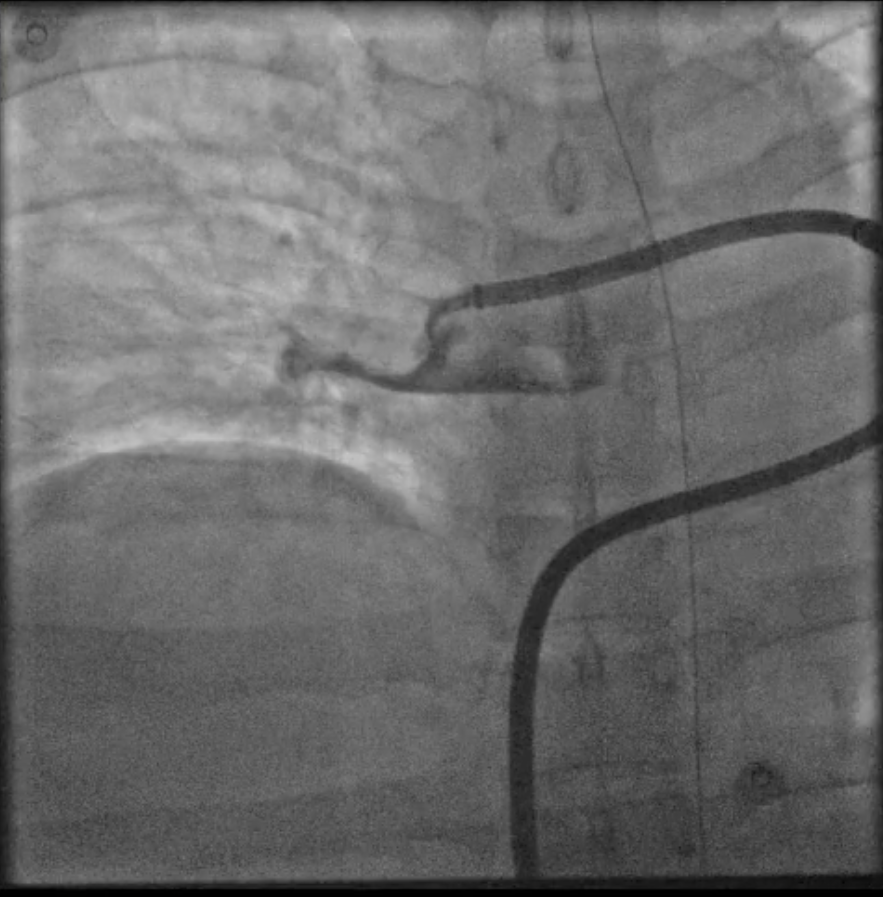
Invasive pulmonary angiogram showed heavy thrombus burden in the right pulmonary artery (Figure B). A brief hemodynamic study was performed, demonstrating a markedly elevated mean pulmonary arterial pressure (mPAP) of 49mmHg.
Interventional Management
Procedural Step
Although she was not hemodynamically compromised, we decided for mechanical thrombectomy as she had demonstrated failure of conservative management with clinical deterioration. While she did not fulfil class I indication for advanced therapies, increasingly we recognize that these patients are at high risk of deterioration and earlier intervention may be needed. Moreover, we are equipped with the Indigo aspiration system which has been shown in the EXTRACT-PE trial to be safe and effective.
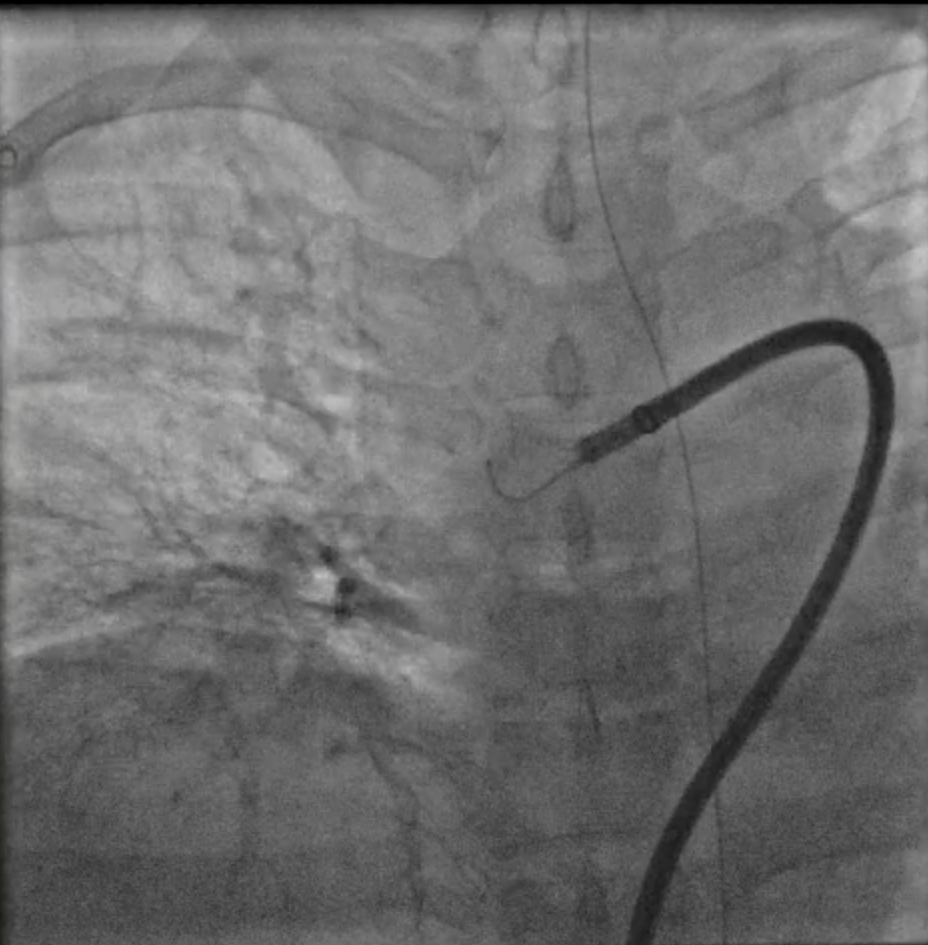
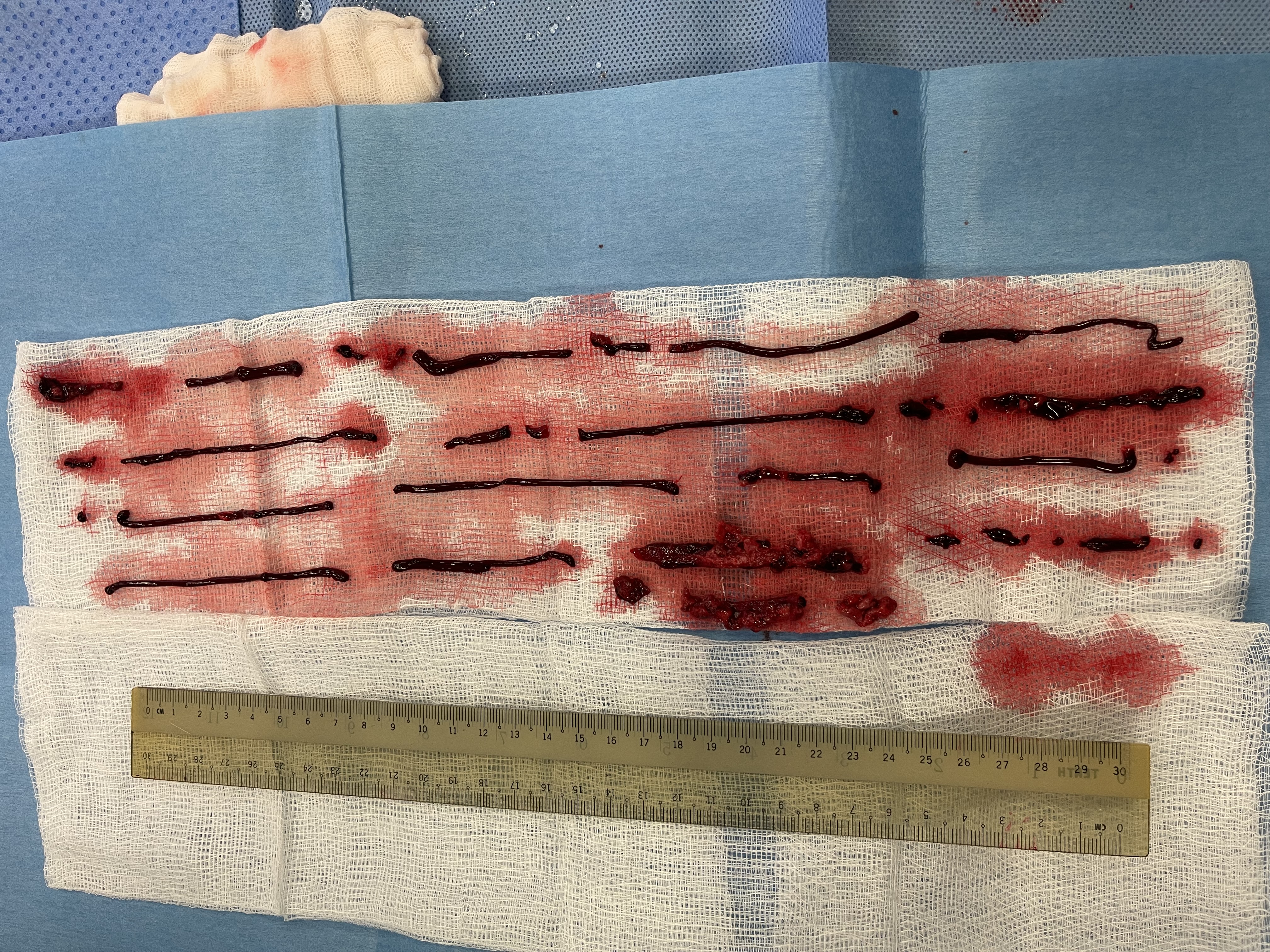
Using the Indigo aspiration system, we conducted multiple runs of aspiration thrombectomy. Initially there was difficulty in aspirating the thrombus, likely due to the size of the extensive right PA thrombus. We then used separator helped to facilitate clot dislodgement and separation (Figure C). We then repeated a few runs of aspiration thrombectomy which yielded large clots (Figure D), many of which were likely recent.
A repeat pulmonary angiogram showed a large reduction in clot burden (Figure E). Immediately after the procedure, the patient's heart rate settled with marked improvement in symptoms and mPAP dropped to 28mmHg.

Using the Indigo aspiration system, we conducted multiple runs of aspiration thrombectomy. Initially there was difficulty in aspirating the thrombus, likely due to the size of the extensive right PA thrombus. We then used separator helped to facilitate clot dislodgement and separation (Figure C). We then repeated a few runs of aspiration thrombectomy which yielded large clots (Figure D), many of which were likely recent.
A repeat pulmonary angiogram showed a large reduction in clot burden (Figure E). Immediately after the procedure, the patient's heart rate settled with marked improvement in symptoms and mPAP dropped to 28mmHg.
Case Summary
In patients with intermediate-high risk PE, it is important to consider advanced therapies early instead of waiting for hemodynamic compromise or development of massive PE, which may portend worse outcomes for the patient. Catheter directed pulmonary thrombectomy will become an increasingly valuable part of the arsenal, especially as more safety and efficacy data becomes available.