
Lots of interesting abstracts and cases were submitted for TCTAP 2023. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-094
Warning: Steep Curve Ahead
By Adelyn Nisha Henry, Muhamad Ali SK Abdul Kader, Kumutha Gobal, Vicknesan Kulasingham, Gurudevan Mahadevan
Presenter
Adelyn Nisha Henry
Authors
Adelyn Nisha Henry1, Muhamad Ali SK Abdul Kader2, Kumutha Gobal1, Vicknesan Kulasingham3, Gurudevan Mahadevan1
Affiliation
Sultanah Aminah Hospital, Malaysia1, Sultan Idris Shah Serdang Hospital, Malaysia2, Ministry of Health Malaysia, Malaysia3,
View Study Report
TCTAP C-094
CORONARY - Complex and Higher Risk Procedures for Indicated Patients (CHIP)
Warning: Steep Curve Ahead
Adelyn Nisha Henry1, Muhamad Ali SK Abdul Kader2, Kumutha Gobal1, Vicknesan Kulasingham3, Gurudevan Mahadevan1
Sultanah Aminah Hospital, Malaysia1, Sultan Idris Shah Serdang Hospital, Malaysia2, Ministry of Health Malaysia, Malaysia3,
Clinical Information
Patient initials or Identifier Number
Mr. C
Relevant Clinical History and Physical Exam
Patient is a 77-year-old Chinese male with a background history of hypertension, dyslipidemia and IHD with CABG done 17 years ago. His grafts are as follows: SVG to OM 3, SVG to PDA, SVG to D1 and LIMA to LAD.He complained of chest pain for the last few weeks. This chest pain was associated with diaphoresis, giddiness, orthopnea and PND. NYHA class 1On examination he was alert and conscious. Not tachypneic and vitals were stable. JVP not elevated. Lungs clear. Cardiovascular system unremarkable
Relevant Test Results Prior to Catheterization
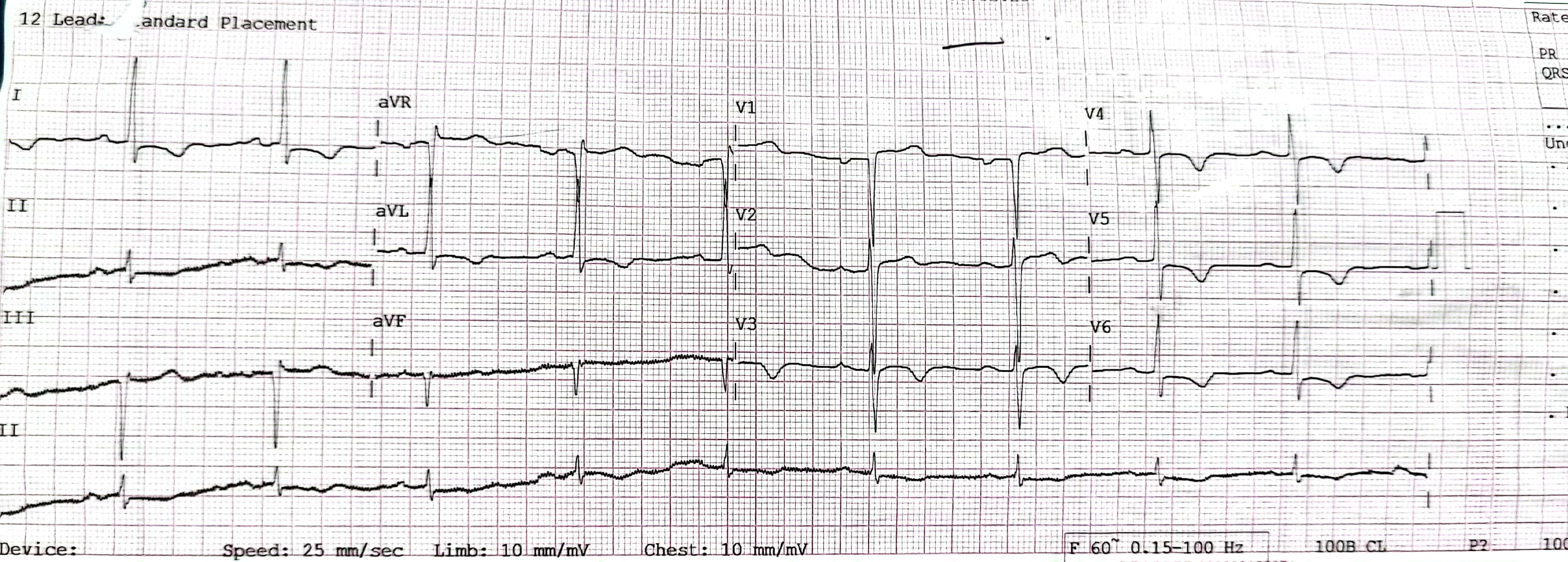
Troponin I 29806.88Creatinine kinase : 234Hemoglobin 11 g/dlCreatinine 83Electrocardiogram: sinus rhythm with t wave inversion 1, AVL, V2-V6Echocardiogram: Ejection fraction :40%, inferoseptal hypokinesia.
Relevant Catheterization Findings
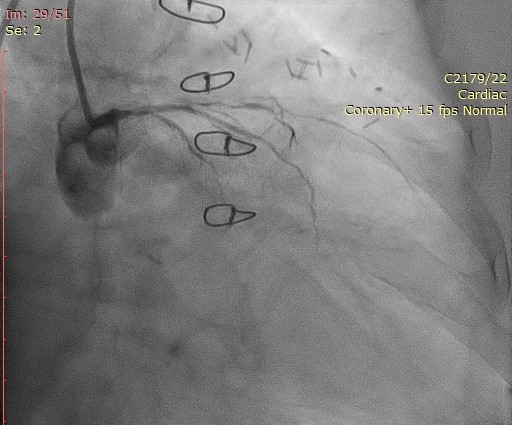
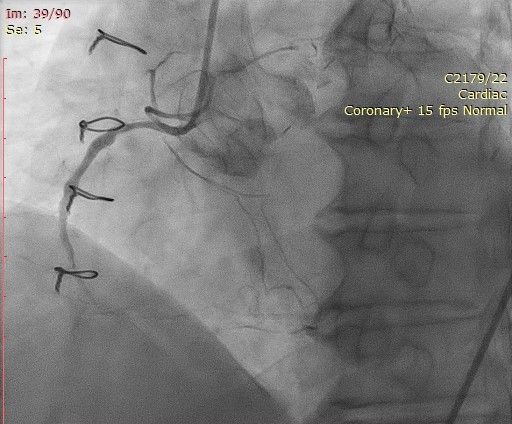
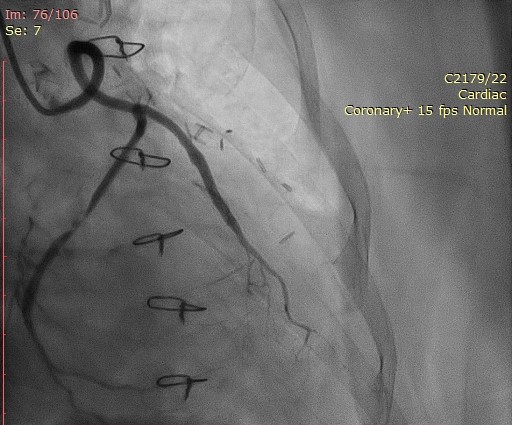
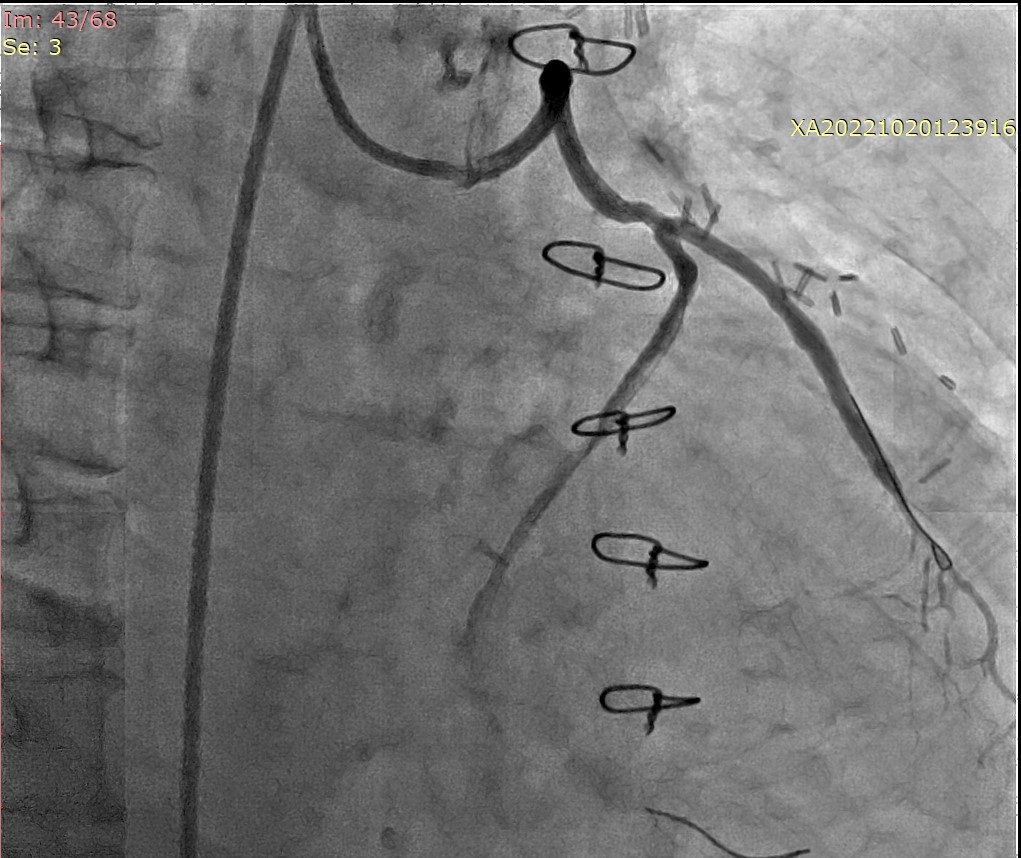
Graft study was performed. There was diffuse disease 99% from the ostial LAD till distal. The LCX was also 99% stenosed from the ostium. The MRCA was a CTO. The SVG to the OM3 had a 80% stenosis in the midsection and the SVG to the PDA had a 50% stenosis in the mid. The SVG to D1 and LIMA to LAD were patent.
Interventional Management
Procedural Step
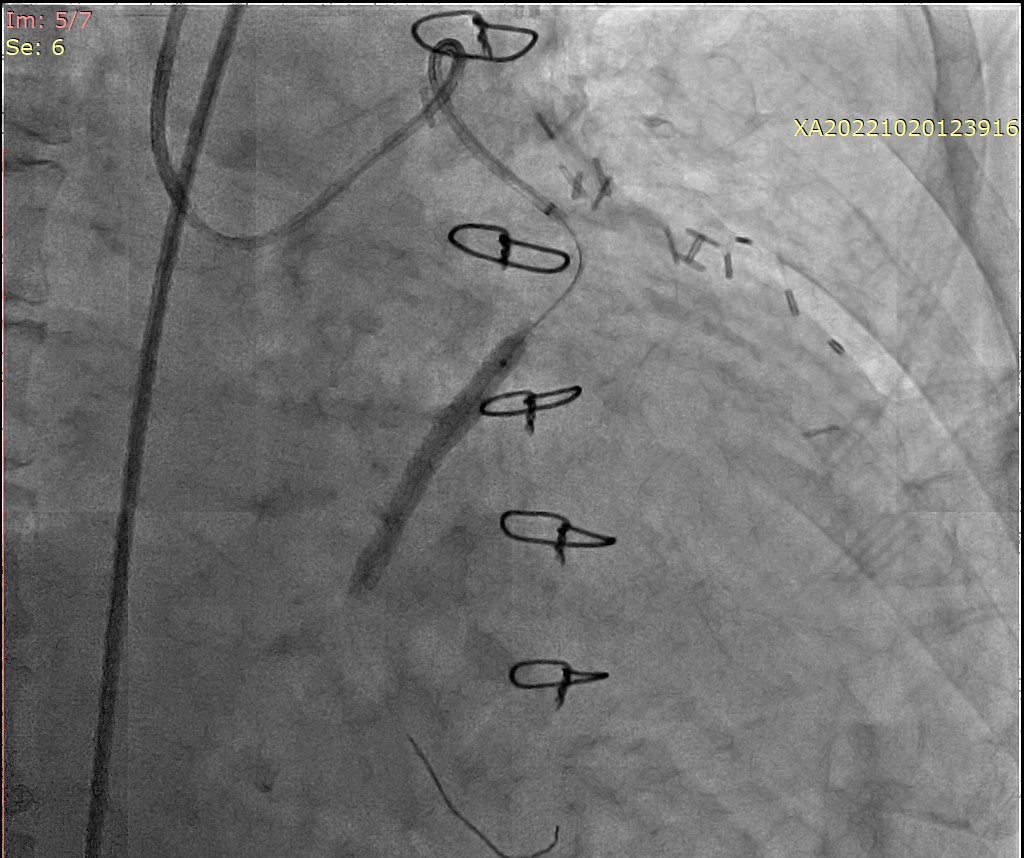
The graft to OM1 was engaged with a JR4 guiding catheter. The SVG to OM was wired with a Runthrough Intermediate. Predilated with a EUPHORA 2.0x15 @ 18atm. We were unable to deliver a RESOLUTE INTEGRITY 2.5x20 stent. We then used a second wire and wired the SVG to D1 with a Sion Blue. The lesion was predilated with a Firefighter 3.5x29 @ 20ATM.Delivery of the stent also failed as it was unable to negotiate the tortuous curve of the graft. Anchor balloon technique was attempted with the FIREFIGHTER balloon inflated in the SVG to D1. Finally with the assistance of a Guide extension catheter, we were able to deliver a FIREHAWK 3.5x29 @ 20atm.IV GTN 300mcg and Intracoronary Adenosine 200mcg were given and there was TIMI 3 flow.
The results were good and patient was discharged home well the next day.
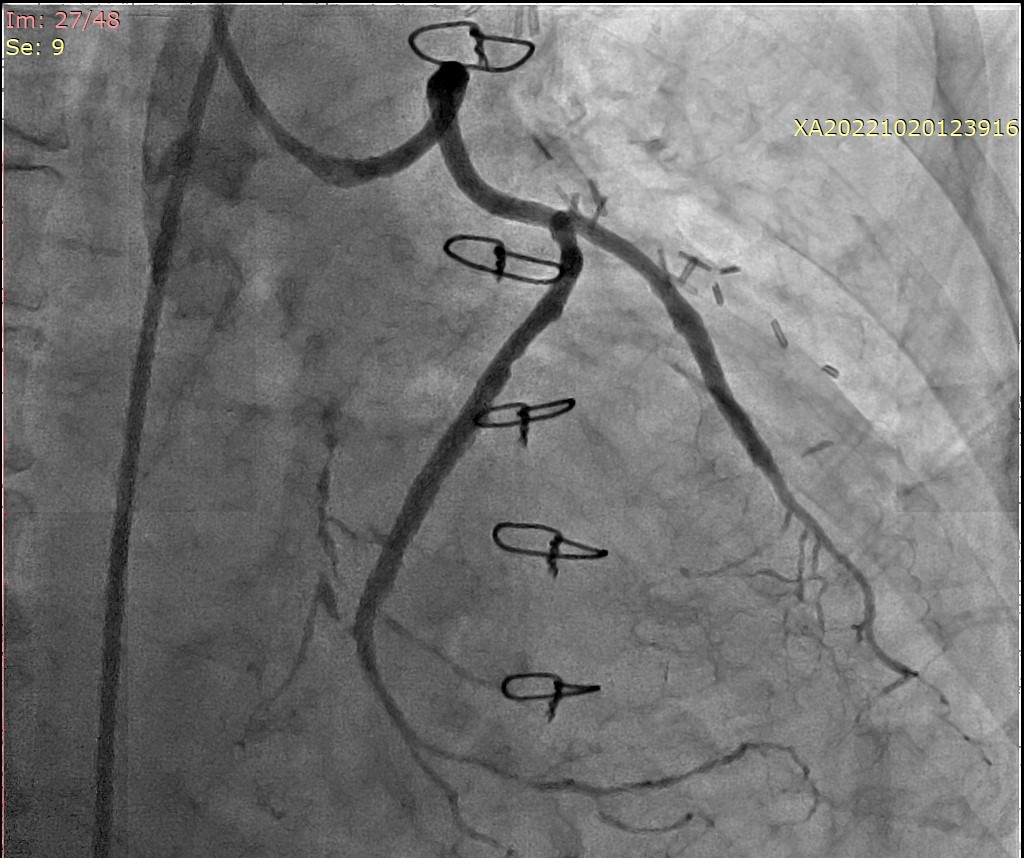
The results were good and patient was discharged home well the next day.
Case Summary
One of the most common causes for stent delivery failure is due to vessel tortuosity. There are several methods documented to assist in stent delivery in these situations and some of them include the buddy wire technique, anchor balloon technique and the use of a telescopic guide. Such problems should be anticipated and alternative strategies should be employed if one or the other fails.