
Lots of interesting abstracts and cases were submitted for TCTAP 2023. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-054
Optimizing DK Crush Stenting in Un-Protected LM Bifurcation
By David Almeidi, Achmad Fauzi Yahya
Presenter
David Almeidi
Authors
David Almeidi1, Achmad Fauzi Yahya1
Affiliation
Dr. Hasan Sadikin Central General Hospital, Indonesia1,
View Study Report
TCTAP C-054
CORONARY - Bifurcation/Left Main Diseases and Intervention
Optimizing DK Crush Stenting in Un-Protected LM Bifurcation
David Almeidi1, Achmad Fauzi Yahya1
Dr. Hasan Sadikin Central General Hospital, Indonesia1,
Clinical Information
Patient initials or Identifier Number
RR
Relevant Clinical History and Physical Exam
A 52-year-old man presented with chronic coronary syndrome. His cardiovascular risk factors were active smoker and hypertension. He was known to have complex coronary lesions and was referred to our hospital for complex PCI after adamantly refused surgical revascularization. His physical examination was normal.
Relevant Test Results Prior to Catheterization
The laboratory findings were within normal limit. The electrocardiogram showed normal sinus rhythm. The echocardiogram revealed normal left ventricular ejection fraction and global normokinetic. The myocardial perfusion imaging (MPI) revealed induced ischemia in anterior and inferoposterior segments with 10.3% of ischemic burden.
Relevant Catheterization Findings
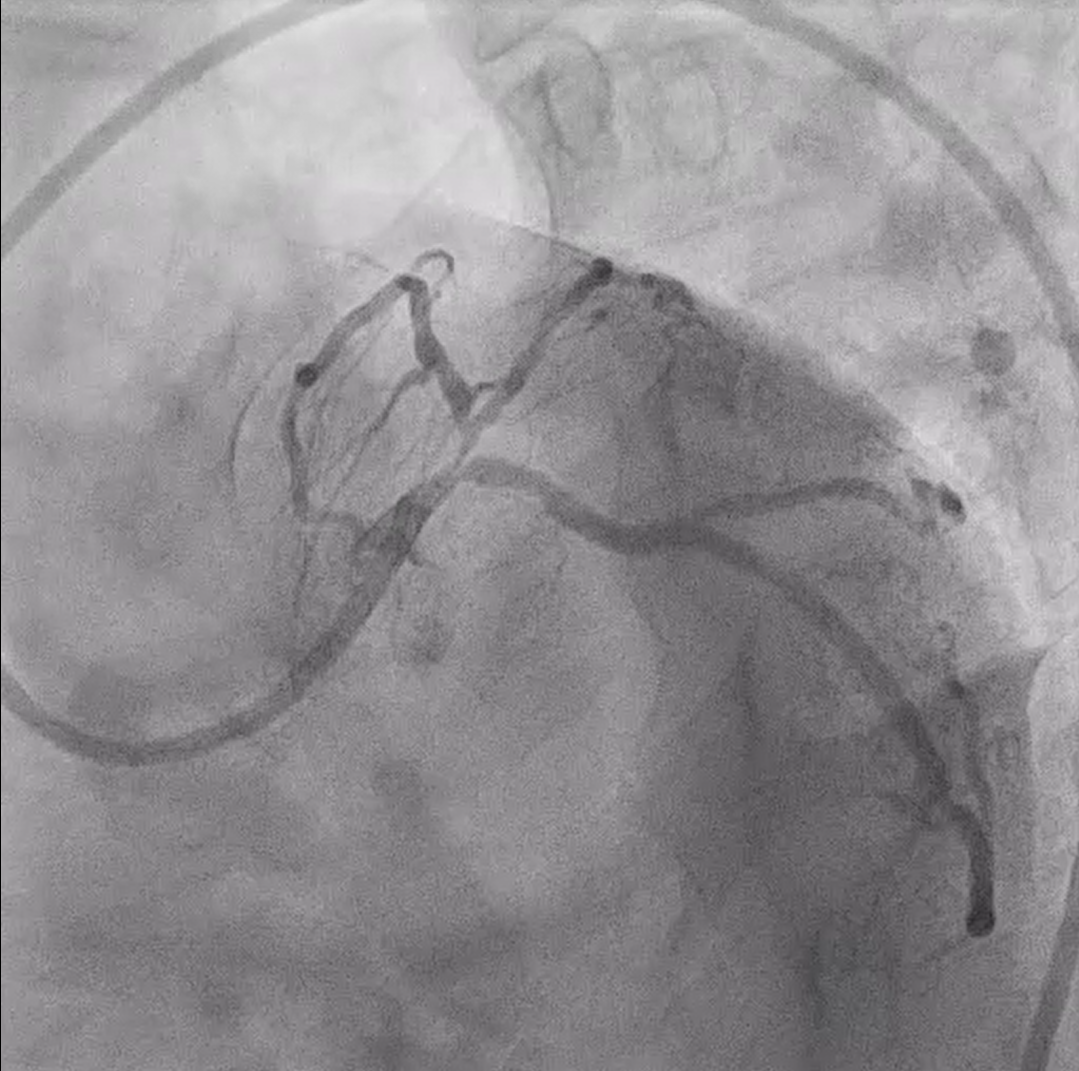
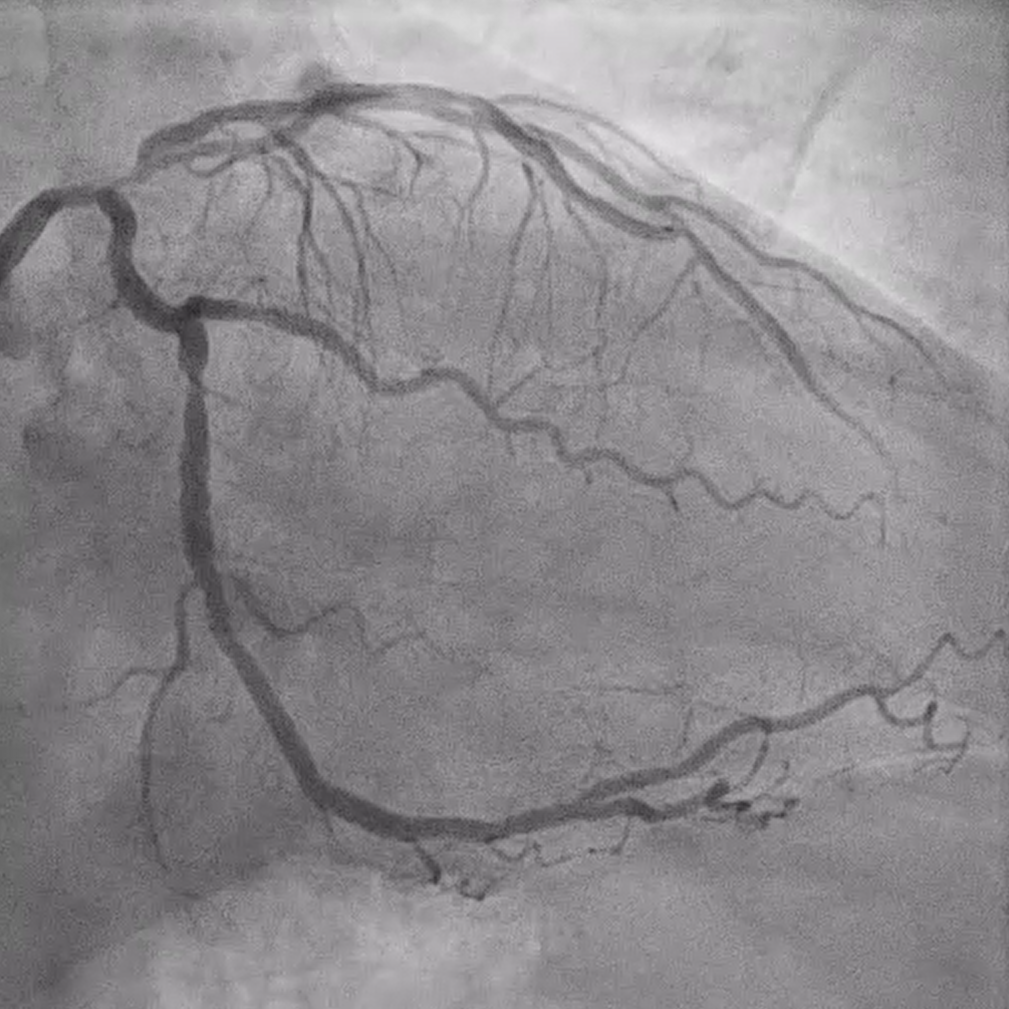
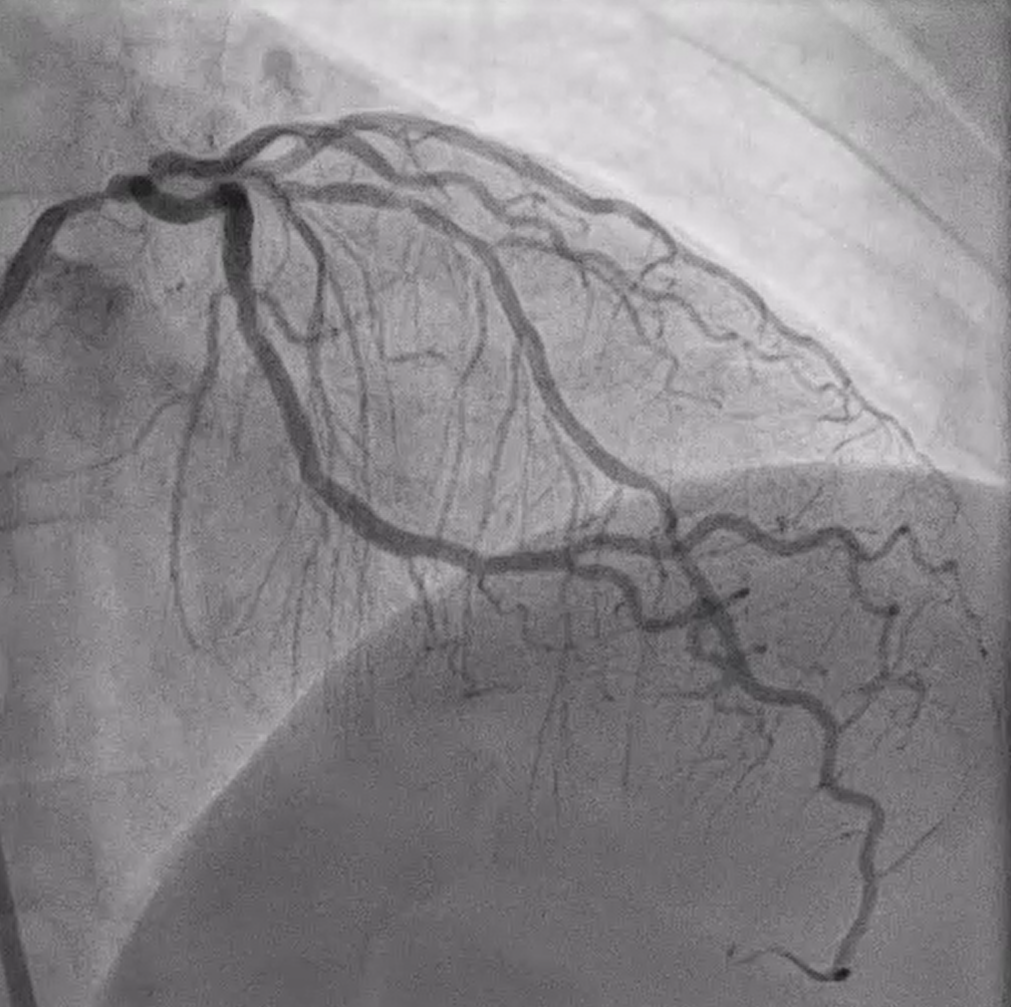
Coronary angiography demonstrated right dominance system, severe left main bifurcation stenosis (Medina 1,1,1). There was severe stenosis at large high Diagonal 1 (D1). The RCA was normal (Figure 1). SYNTAX score 31, EuroScore II 0.5%, STS score 0.36%.
Interventional Management
Procedural Step
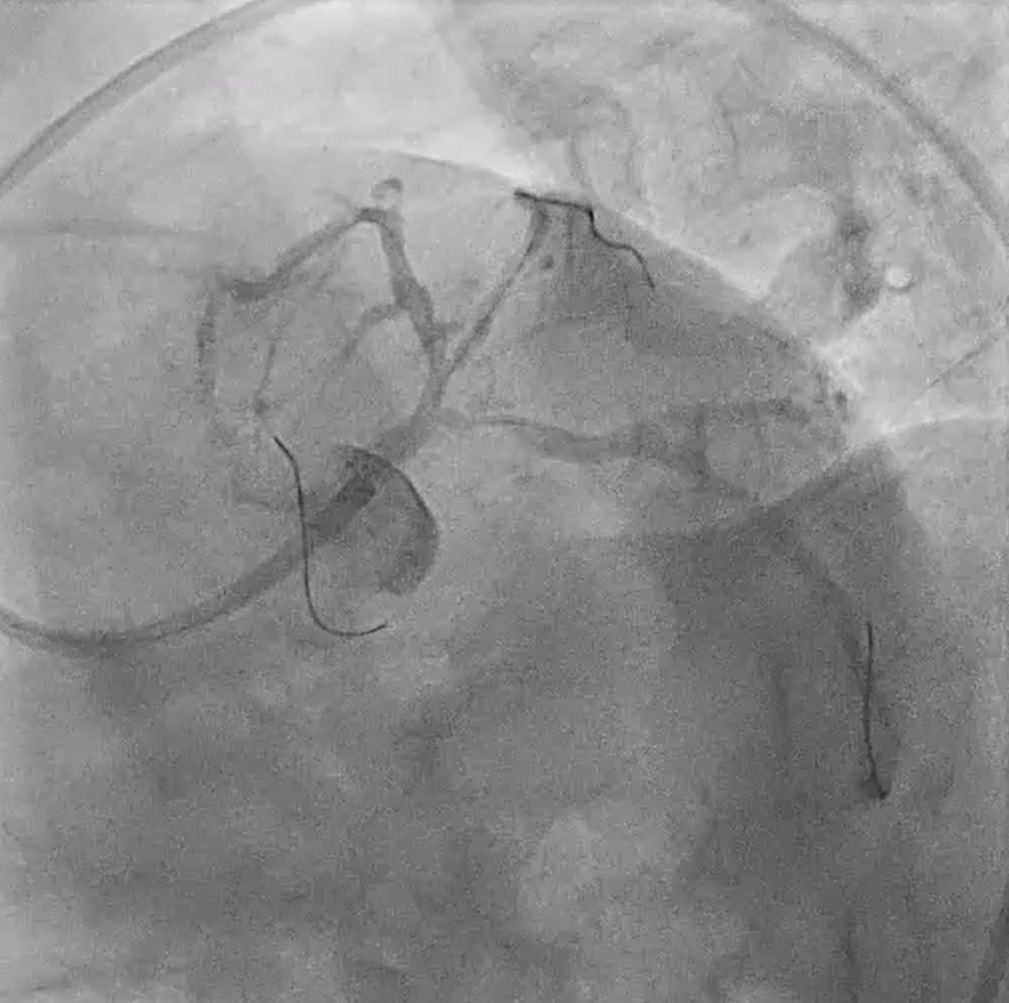
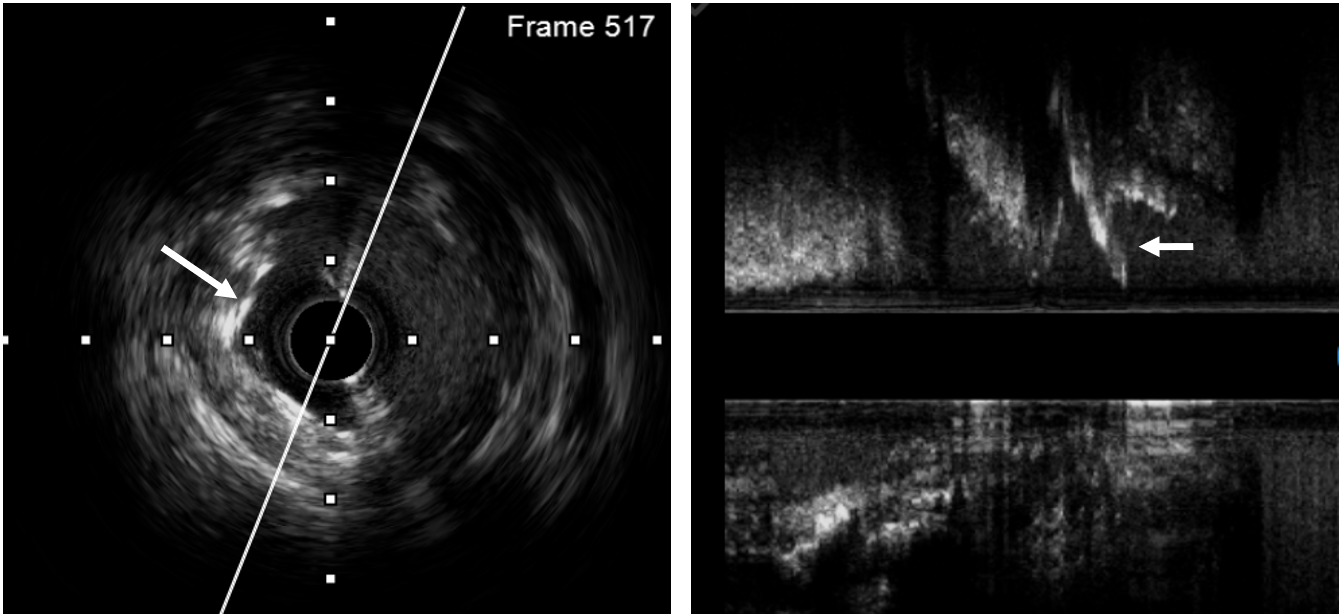
We used 7 Fr EBU guide catheter via right femoral artery. IVUS revealed eccentric fibrotic plaque in LM, LAD and LCx. Initial plan was LM-LAD crossover stenting. LM-LAD was predilated using a 3.0 x 15 mm NCB. Concerning potential compromised of ostial LCX during LM-LAD stenting, LCx was predilated using 3.0 x 15 mm Scoreflex(OrbusNeich®, Hongkong). Unfortunately, ostial LCX was dissected and forced us to switch to 2-stents strategy.

Case Summary
Preserving the side branch is one of the most important aspects in deciding appropriate approach for bifurcation stenting. Upfront-1-stent strategy should be the first approach in non-complex bifurcation lesion while it should always be layered with other strategy as bailout. In this case, as the LMB lesion turned into a complex situation after lesion preparation that result from significant dissection of ostial side branch, we therefore needed to adapt immediately to the situation by switching to DK-crush technique. We used IVUS to optimize the procedure.