
Lots of interesting abstracts and cases were submitted for TCTAP 2023. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-156
Nightmare Case Sharing: Successful Rescue of Right Iliac Artery Rupture
By Chung-Ho Hsu, Kee Koon Ng
Presenter
Kee Koon Ng
Authors
Chung-Ho Hsu1, Kee Koon Ng1
Affiliation
China Medical University Hospital, Taiwan1,
View Study Report
TCTAP C-156
ENDOVASCULAR - Peripheral Vascular Disease and Intervention
Nightmare Case Sharing: Successful Rescue of Right Iliac Artery Rupture
Chung-Ho Hsu1, Kee Koon Ng1
China Medical University Hospital, Taiwan1,
Clinical Information
Patient initials or Identifier Number
Mr. L
Relevant Clinical History and Physical Exam
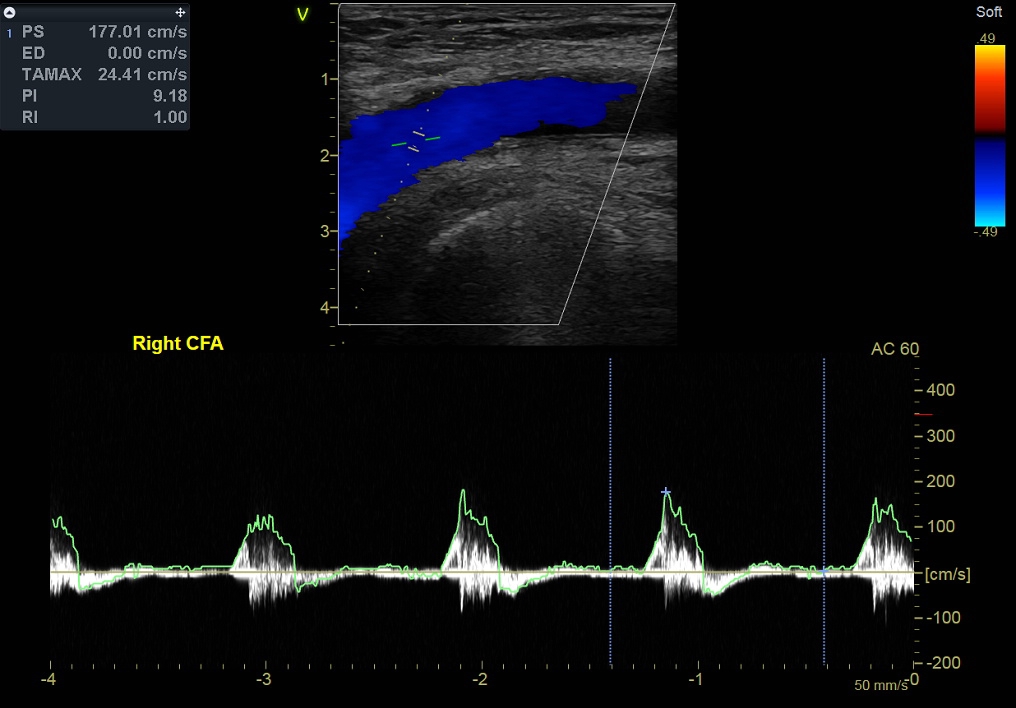
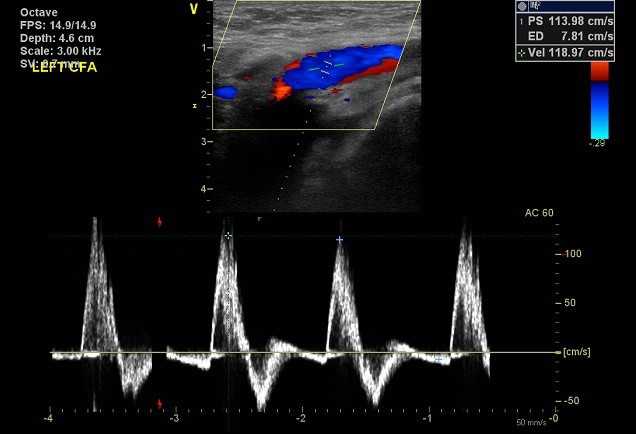
This is a 66 years old male, with BMI 33kg/m2. He experienced low back pain with radiation to right leg since 6 years ago. Lumbar spine MRI revealed degenerative change of L5-S1 with disc space narrowing with no sign of Herniated Intervertebral Disc (HIVD). A peripheral echography revealed decreased blood flow on right common femoral artery. He underwent regular OPD follow up for 4 years until right leg claudication aggravated.

Relevant Test Results Prior to Catheterization
Serial CT scan images revealed no contrast enhancement of right external iliac artery. Total occlusion is highly suspected.


Relevant Catheterization Findings
A 6Fr Cook crossover sheath was inserted via Left Common Femoral artery (LCFA) toRight Common Iliac Artery (RCIA) under echo-guidance, followed by micropuncture, V18, 4Fr sheath and Roadrunner wire. Judkins 4 catheter was used. Total occlusion of right external iliac artery was confirmed.



Interventional Management
Procedural Step
Antegrade wiring with V18/CXI was failed. Another attempt was made with retrograde wiring with V18/CXI via 4 Fr sheath inserted to Right Common Femoral Artery (RCFA), still failed. Double balloon technique was used. Balloon dilatation catheter of size 3.0/40 mm and 3.0/80 mm Armada were inflated with 6-8 atm. Then, 3.0/40 mm and 4.0/80 mm Armada with 8 atm were attempted. But, failed wiring. The balloon dilatation catheter was upsize to 4.0/80 mm Armada and 5.0/40mm Admiral inflated with 6 atm. The patient developed hypotension with Systolic Blood Pressure (SBP) of 80 mmHg and tachycardia. External iliac artery perforation was confirmed by contrast extravasation at proximal external iliac artery (Figure A). Blood pressure was stabilized at SBP of 120 mmHg after Admiral 5.0/40mm balloon inflation, normal saline hydration and norepinephrine pump infusion. A 8.0/50mm Heparin coated Viabahn graft stent (V3H) was deployed via 7 Fr Crossover. Externalization with 20 mm Snare was performed. Zilver stents of size 8.0/60 mm and 10.0/40 mm were deployed on both openings overlapping with previously placed V3H stent, post-dilated with 6.0/80 mm and 7.0/80 mm Admiral at 8-10 atm. Antegrade injection of contrast revealed good flow (Figure B). An aneurysmal dilatation of distal Right Iliac Artery (RIA) was notable. A V3H stent with size of 7.0/50 mm was placed, post-dilated with 7 mm balloon at 3 atm. Residual stenosis was 0% with TIMI-3 flow achieved as indicated by retrograde contrast injection (Figure C)



Case Summary
For the intervention on iliac artery chronic total occlusion, it is strongly suggested that graft stent must be make available in catheter laboratory in case of catastrophic iliac artery rupture. In this case, iliac extravasation resulting in hypovolemic shock developed after double balloon technique. The perforation was successfully sealed with Viabahn covered stent. Successful wiring and externalization was achieved after this catastrophic event.