
Lots of interesting abstracts and cases were submitted for TCTAP 2023. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-115
Severe Dissection Post DCB, DK Crush to the Rescue
By Boon Cong Beh, Mohd Asyiq Al-Fard Bin Mohd Raffali, Noor Diyana Binti Mohamad Farouk, Shawal Faizal Mohamad
Presenter
Boon Cong Beh
Authors
Boon Cong Beh1, Mohd Asyiq Al-Fard Bin Mohd Raffali1, Noor Diyana Binti Mohamad Farouk1, Shawal Faizal Mohamad1
Affiliation
Hospital Canselor Tuanku Muhriz UKM, Malaysia1,
View Study Report
TCTAP C-115
CORONARY - Complications (Coronary)
Severe Dissection Post DCB, DK Crush to the Rescue
Boon Cong Beh1, Mohd Asyiq Al-Fard Bin Mohd Raffali1, Noor Diyana Binti Mohamad Farouk1, Shawal Faizal Mohamad1
Hospital Canselor Tuanku Muhriz UKM, Malaysia1,
Clinical Information
Patient initials or Identifier Number
MAFA
Relevant Clinical History and Physical Exam
A 33-year old man, who was chronic heavy smoker, with underlying morbid obesity and obstructive sleep apnea (OSA) presented with sudden onset of left sided chest pain at rest and associated with breathlessness. He presented to emergency department for further evaluation. Hemodynamic stable upon arrival and clinical examination was unremarkable.
Relevant Test Results Prior to Catheterization
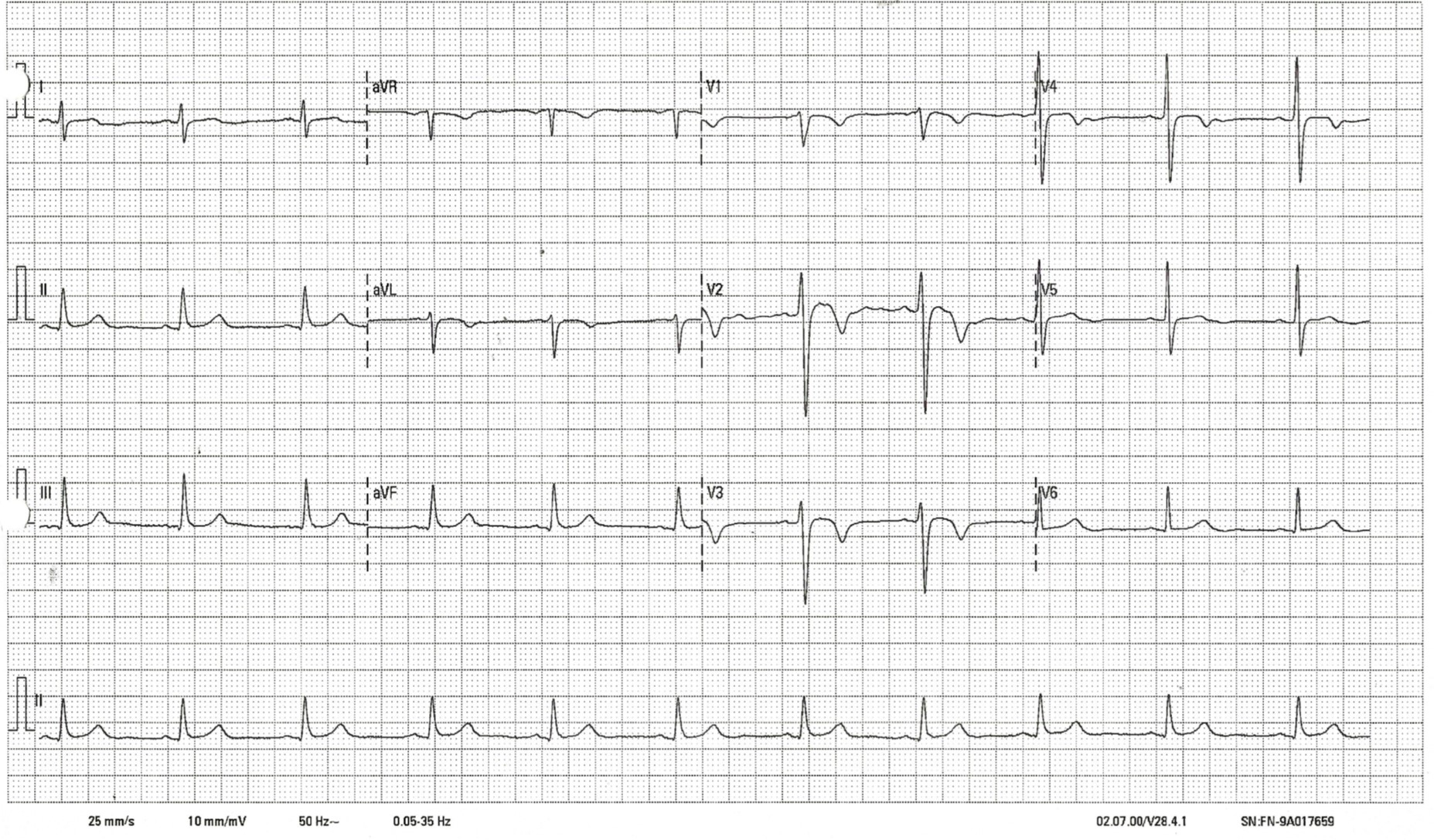
Serial electrocardiograms showed dynamic T waves changes in antero-septal region (Wellen’s syndrome). His serial Troponin I were increased (highest 437pg/ml).
Relevant Catheterization Findings
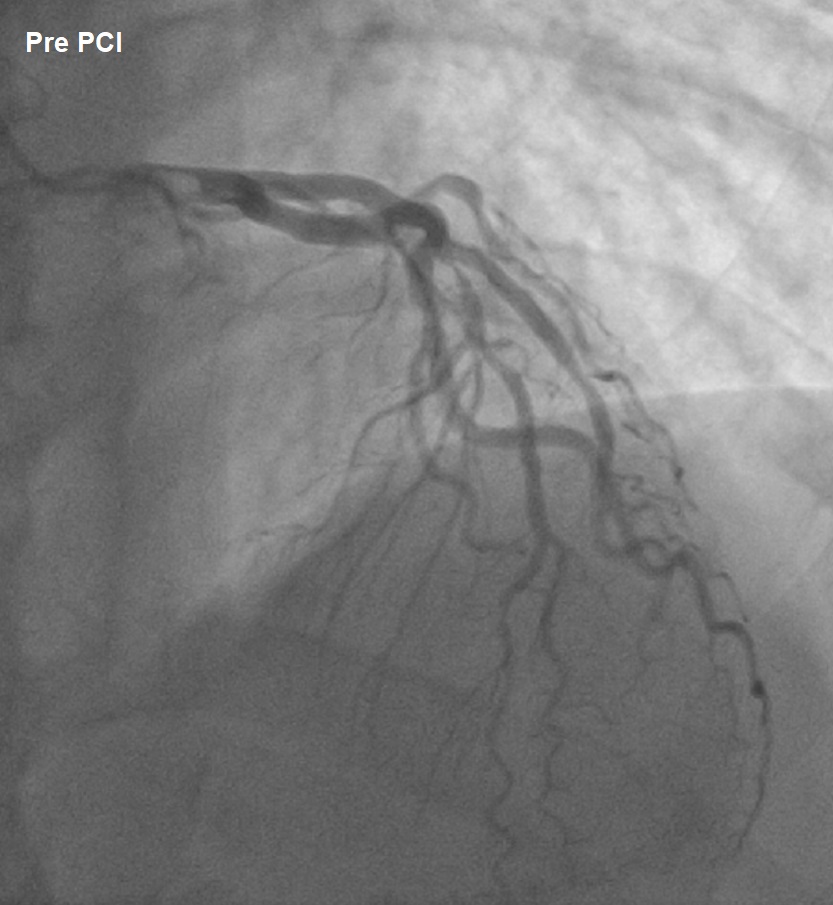
LMS : Unobsturcted
LAD : Midsegment bifurcation disease (1,1,0), big septal branch with ostial-proximal 95% disease(truncated)
LCx : Mild disease, OM 50% disease
RCA : Mild disease.
LAD : Midsegment bifurcation disease (1,1,0), big septal branch with ostial-proximal 95% disease(truncated)
LCx : Mild disease, OM 50% disease
RCA : Mild disease.
Interventional Management
Procedural Step
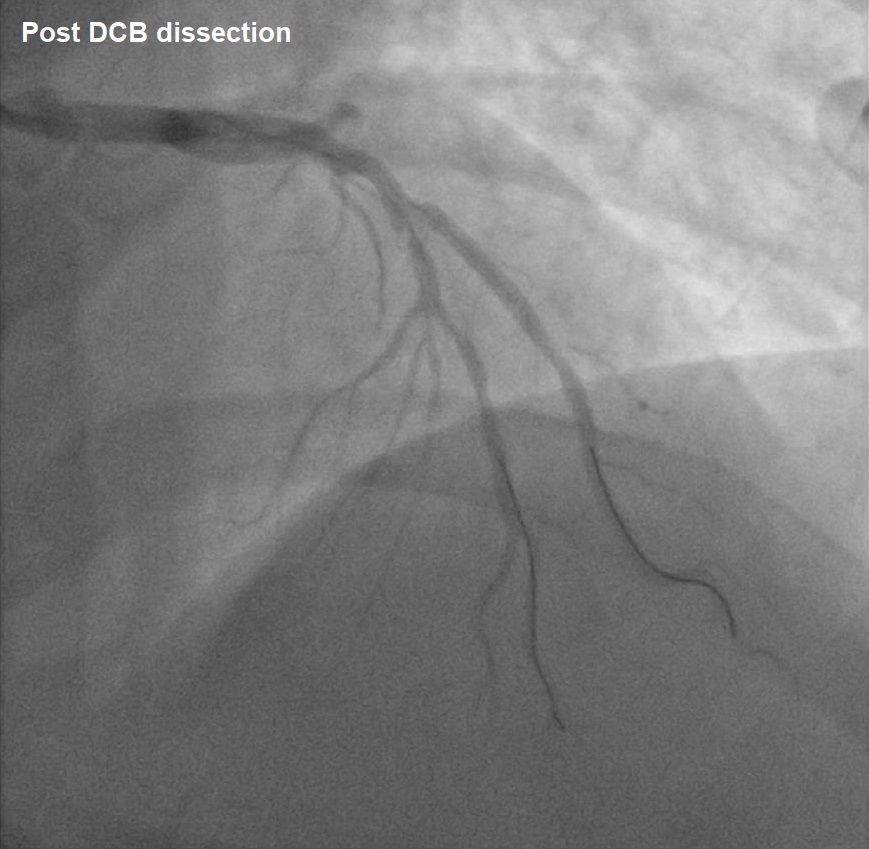
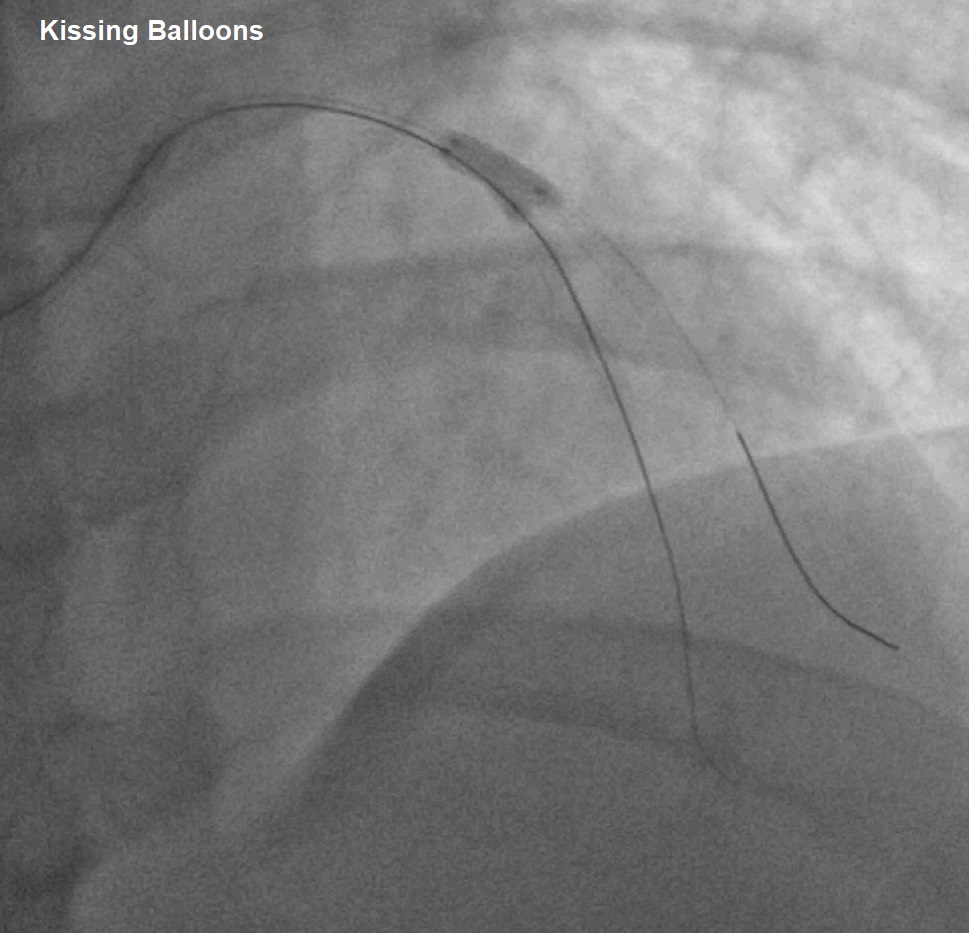
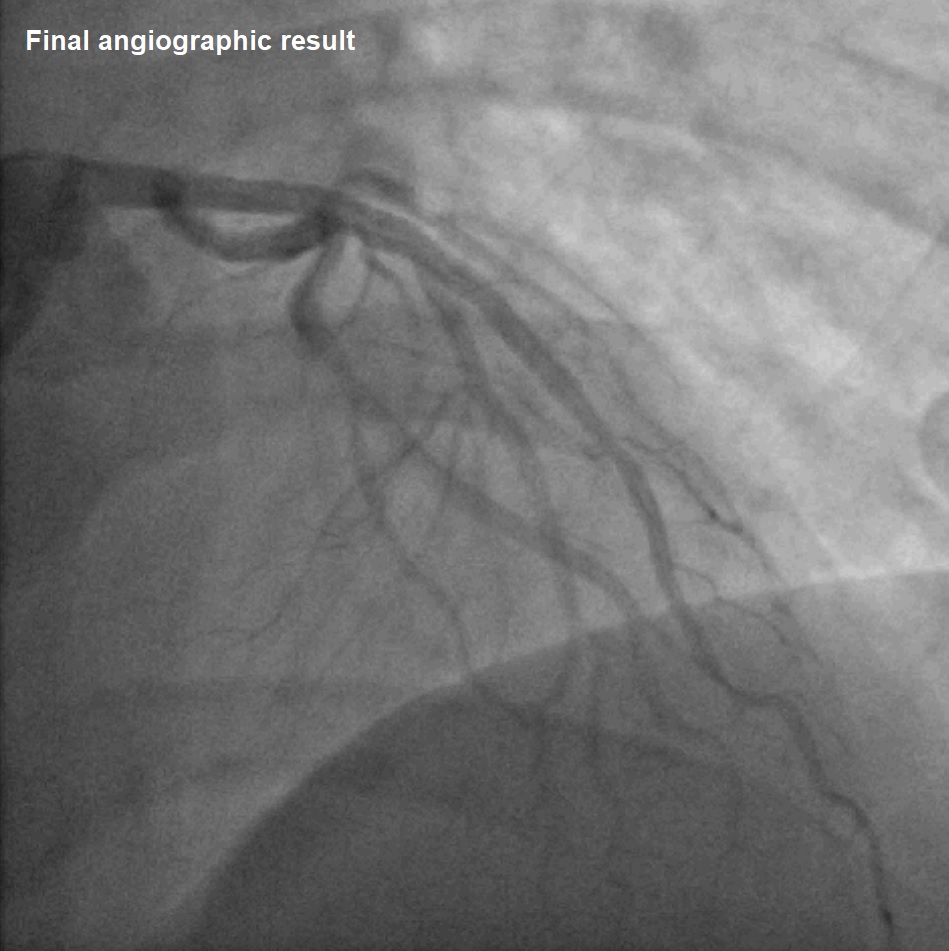
Right radial artery access, and the LCA was engaged with 6Fr EBU 3.0 guiding catheter. Initial strategy was provisional DCB angioplasty of bifurcation lesion (1,1,0) of the truncated LAD. 1st coronary guidewire was introduced and crossed to truncated septal branch, and another guidewire was anchored at LAD. Lesion was predilated with semi compliance balloon 2.0x15mm (nominal), however, noted linear dissection(type B). Subsequently treated with DCB 2.0x20mm(6atm, 55seconds), noted worsening of dissection at septal branch (Figure A). with >70% recoiled. Hence, decided for bail-out with DK crush technique. Due to limited space for multiple wires and balloons to passthrough, sheath was changed to Terumo Glidesheath Slender 7Fr. Bifurcation lesion (Septal) stented with drug-eluting stent (DES)2.5x23mm(6atm). Rewired to distal septal, and subsequently 1st kissing balloons done with non-compliance(NC) balloon 2.5x15mm (12atm) for Septal and 3.0x15mm (12atm) for LAD. Proceeded with LAD stenting with DES 2.5x28mm(11atm). Followed by rewired with Fielder XT to distal septal branch through the stent strut and 2nd kissing balloons with NC balloon 2.5x10mm(14atm) for LAD and 3.0x10mm(14atm) for LAD(Figure B). Final proximal optimisation technique (POT) of LAD stent with NC balloon3.5x10mm (12atm). Post procedure good angiographic result. Post procedure he remained asymptomatic and discharged well after 3 days monitoring.
Case Summary
Two-stents strategy should be considered for bailout in provisional stenting strategy for bifurcation lesion. Culloute, TAP, DK Crush or reverse DK crush strategy should be considered when significant side branch compromised based on the preference of interventionalist.